Event - ThyCa
Find your care
We deliver effective, minimally invasive treatments in a caring environment. Call 310-267-7838 to connect with an expert in endocrine surgery.
UCLA physicians gave talks at the recent 19th International Thyroid Cancer Survivors' Conference.
ThyCa is a patient-centered organization that provides education and support for thyroid cancer survivors.
Dr. Gregory Brent answered questions about Thyroid Hormone Replacement, including dosing and medication options.
Dr. Angela Leung discussed Thyroid Cancer in Pregnancy. It is unclear whether pregnancy stimulates thyroid nodules to grow.
If it is indicated, a biopsy can safely be done of the thyroid nodule during pregnancy. Surgery for thyroid cancers discovered during pregnancy may usually be delayed until after delivery and breastfeeding are complete.
After surgery, radioactive iodine ablation may be indicated in some patients, but this treatment cannot safely be given during pregnancy or while breastfeeding.
Dr. Stephanie Smooke summarized The American Thyroid Association (ATA) 2015 Guidelines on Thyroid Nodules and Differentiated Thyroid Cancer, and Dr. Masha Livhits discussed Initial Surgery for Thyroid Cancer.
Drs. Smooke and Livhits emphasized that most (although not all) thyroid cancers are slow-growing and not very aggressive. Therefore, the management of thyroid nodules and tumors should also not be overly aggressive.
The recent ATA guidelines recommend that only thyroid nodules larger than 1 cm should be biopsied in most cases. A physician experienced in thyroid ultrasound should look at the appearance of the thyroid nodule on ultrasound and determine whether a biopsy is required.
The guidelines also suggest that many smaller thyroid cancers up to 4 cm can be treated with thyroid lobectomy alone (removing half of the thyroid).
This allows the patient to keep the other half of their thyroid and potentially avoid the need for thyroid hormone medication.
Dr. Michael Yeh shared his extensive experience with Reoperation for Recurrent Thyroid Cancer. Most patients are fully treated after one good, comprehensive operation. Preoperative ultrasound is critical to identify all sites of disease in the thyroid gland as well as the lymph nodes in the neck, so that the entire tumor can be removed during the initial surgery.
Despite this, some patients will have a recurrence either due to an inadequate initial surgery or more aggressive disease biology. An elevated tumor marker (thyroglobulin) is often the first clue that a thyroid cancer has recurred.
The next step is imaging, again relying primarily on ultrasound to look for an abnormal nodule or lymph node in the neck. A biopsy is then performed to confirm thyroid cancer.
At all points during the investigation, the benefits of a potential reoperation must be carefully weighed against the increased risks of surgery in a scarred field.
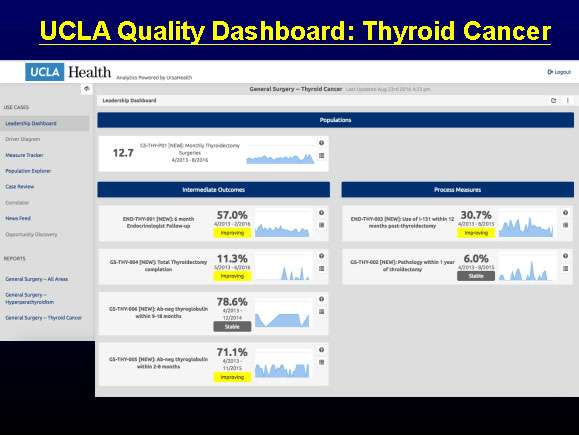
At UCLA, we follow all of our patients for at least one year following their thyroid cancer surgery (see Quality Dashboard below).
We track outcomes including tumor markers and recurrence rates to ensure that we are delivering the best care for our patients.