Example of Change to Nerve Sparing
Find your care
Our radiologists lead the way in prostate imaging. We offer the newest techniques to better detect and stage prostate cancer. Call 310-481-7545 to find out more about prostate imaging and treatment options.
History
- 59 year-old
- PSA 4.3
- standard biopsy: 3+3=6 but large volume left
Imaging
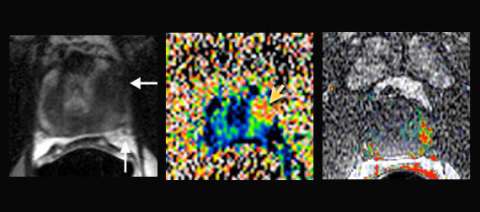
LEFT: T2-weighted imaging: hypointense focus left anterior apex (horizontal arrow) with uninvolved neurovascular bundle (vertical arrow)
CENTER: Colorized apparent diffusion coefficient (ADC) map: moderately restricted diffusion (yellow arrow)
RIGHT: Colorized dynamic contrast enhanced (DCE) perfusion map: focal intense enhancement
Example Report for This Case: Surgical Planning
* Findings
No suspicious lymph nodes or bone lesions. Prostate measures 38 gm with mild prostatic hyperplasia. A single suspicious area is identified:
| Location | Left anterior central apex 2:00 |
| Capsule | Bulges anteriorly only |
| T2 | Asymmetric, ill-defined (4/5) |
| Diffusion | ADC 0.82, highly restricted (4/5) |
| Perfusion | Early and intense + washout (4/5) |
| Spectroscopy | Abnormal |
| Overall Suspicion | High (4/5) |
Seminal vesicles and neurovascular bundles appear normal.
* Impression
- Technical quality: excellent
- Left anterior lesion highly suspicious for aggressive disease may involve anterior capsule
- Organ-confined disease.
Result
Final Path: 3+4=7, T2c
Advantage: UCLA Prostate MRI
- In cases of suspected high volume but organ confined disease, MRI can help with the decision to spare one or both nerves and still achieve negative surgical margins
- Spectroscopic imaging is the most specific of the functional parameters of prostate MRI, but requires focused experience to accurately tune the magnet