Indeterminate Thyroid Nodule
Find Your Care
We deliver effective, minimally invasive treatments in a caring environment. Call 310-267-7838 to connect with an expert in endocrine surgery.
What is an indeterminate thyroid nodule?
An indeterminate thyroid nodule is a growth within the thyroid gland that could possibly be cancerous. About 25% of indeterminate thyroid nodules are ultimately found to be cancers.
Molecular Testing of Thyroid Nodules
UCLA endocrine surgeons Masha Livhits, MD & James Wu, MD, presented a webinar to discuss molecular testing of thyroid nodules.
UCLA Endocrine Surgeons Featured in National Comprehensive Cancer Network Video on Molecular Testing for Thyroid Nodules
UCLA Endocrine Center physicians Drs. Masha Livhits and Michael Yeh discuss their latest study on molecular testing for indeterminate thyroid nodules. We compare new genetic tests that help us tell the difference between benign and possibly cancerous thyroid nodules. Patients with benign test results can avoid unnecessary thyroid surgery.

Video: Drs. Yeh & Livhits - Predicting the Risk of Malignancy in Thyroid Nodules | View Video Transcript
Summary
About 25% of the time when we biopsy a thyroid nodule, we will diagnose it as an “indeterminate thyroid nodule.” This is when the cells do not look completely benign but also do not look absolutely cancerous. Nodules in this grey area have a 5-30% chance of containing a thyroid cancer. In the past, we would perform surgery on all indeterminate thyroid nodules to avoid missing a cancer diagnosis. Unfortunately, many patients found out after surgery that their thyroid nodule was actually benign.
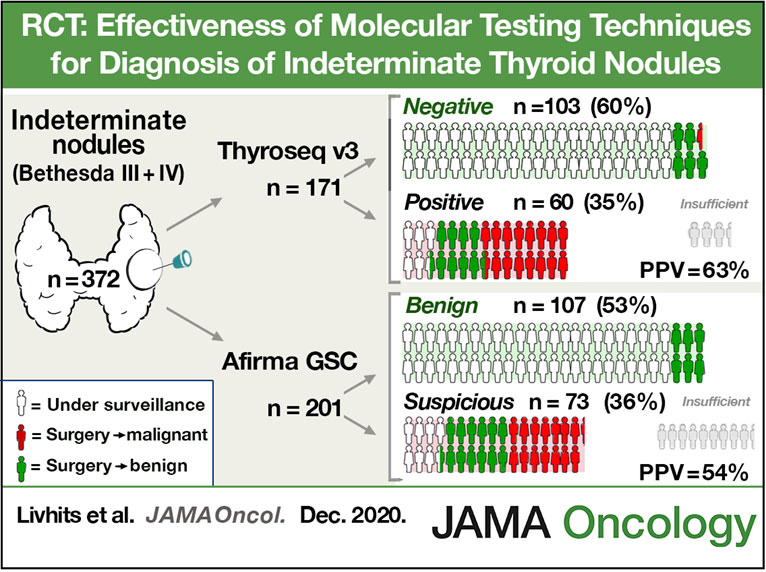
Now, molecular tests can help us predict whether an indeterminate nodule will be benign or cancerous. In this study we compared the newest version of the two most prominent molecular tests, Thyroseq V3 and Afirma Gene Sequencing Classifier.
Although both tests work in different ways, their accuracy and performance were roughly the same. About 50-60% of the patients we test get a benign result. The remaining patients get a “suspicious” result. When there is a suspicion for cancer, the tests differ slightly. Thyroseq provides a report on DNA mutations present in the tumor. Some mutations, or combinations of mutations, make the cancer behave more aggressively. When we have that information, we can tailor the treatment to the disease. In some patients we may recommend more extensive surgery or radioactive iodine treatment if high-risk mutations are identified.
Watch Video: Molecular Markers for Thyroid Cancer - Masha Livhits, MD & Michael Yeh, MD >
Transcript of Video
[Michael Yeh] Hi. Thanks, Masha, for joining us today. We are here to talk about molecular testing for indeterminant thyroid nodules which make up about 25% of all thyroid biopsy results. Can you tell us a little bit about your study why did you perform an orient test with two molecular test you used?
[Masha Livhits] Sure. So, as you mentioned, about 25% of thyroid nodules have indeterminant cytology. And in that case, it difficult for us to know clinically how to manage those patients. We want to avoid unnecessary diagnostic surgery, and so that I would say the two leading molecular test technologies, are the ones that we studied, which are the Thyroseq V3, and Affirma GSC.
[Masha Livhits] And Thyroseq V3 replies on DNA and RNA based testing. And it gives us a specific mutational information via which mutation was identified in that nodule. And the Affirma GSC is mRNA based and relies on machine learning algorithms. So ultimately that will tell us what is the risk of malignancy, looking at the wide expression of mRNA.
[Michael Yeh] Great. Your study had a unique design with block randomization. Can you tell us a little bit about that?
[Masha Livhits] Yes, so we want to compare the diagnostic performance of these two tests, using the same study population, the same institution, the same centralized site of pathology, and the same prevalence of malignancy. And so we randomized patients, to either receiving one or the other molecular test. Now logistically this is quite challenging, because we have a large institution with several people doing biopsies. That’s one of the strengths of our study with a lot of thyroid FNAs performed every year, over 1,000 annually. Randomizing at the individual patient level was challenging. So instead we randomized patient blocks by months. So, every month we would either do one molecular test and next month switch to the next molecular test.
[Michael Yeh] Masha can you summarize the findings of your study?
[Masha Livhits] Yes. So the first important part of how these tests performed is what is the benign call rate? So, in how many cases will the molecular test return a benign result which is really one of the main utilities of this molecular test, because it allows patients to then avoid diagnostic surgery when the test is benign. So, the findings were that the benign call rate of Affrima GSC and Thyroseq V3 were similar. About 50%-60% of patients had a benign result. So the positive predictive value of the two tests were also similar, about 50%-60% for Affrima GSC and Thyroseq V3. So ultimately, we found that the diagnostic performance of the two tests were very similar.
[Michael Yeh] These are relatively new versions of these two tests, new generations. How does the current test perform to the prior generation test?
[Masha Livhits] Great question. So, we had the opportunity to study the prior test versions, which are affirma GEC and Thyroseq V2. We had performed a similar randomization study using the same study design. And at the point with the prior test iterations, we had found that Affirma GEC had a slightly lower positive predictive value compared to Thyroseq V2. So now when we repeated with the new test versions, which are the ones clinically used in practice, we found that the positive predictive value of affirma increased a little bit from GEC to GSC. While Thyroseq remained fairly similar. So that although the previous test seemed like there was a little bit of a difference in the positive predictive value, the current test versions are very similar.
[Michael Yeh] Great. We talked a lot about the diagnosis of the thyroid nodules that tare indeterminant. What about prognostic value? In other words, if it is a cancer, do these molecular tests tell you how bad of a cancer, how aggressive this could have been?
[Masha Livhits] I think this is one of the most exciting parts of this type of technology, which is “can we used it for prognosis?” And now Thyroseq, as I have mentioned gives the specific mutation that is identified within the thyroid nodule, which is really important for prognosis. For example, thyroid cancers that have a combination of TERT and BRAF V600E mutation. Those are known to really have an increased chance of even mortality related to the thyroid cancer. And that information is known with Thyroseq. Now most nodules that have aggressive mutations, they will have a malignant cytology result. So, they don’t even get necessarily sent off for molecular testing. However, even within the indeterminant cytology nodules, some of them will have these more aggressive mutations. And we have the opportunities to discover that and perhaps manage those patients in a different way, to a little bit more aggressive with surgery, or perhaps additional treatments Radiative Iodine Ablation. On the other hand, we know that thyroid nodules that have Ras mutations are often fairly indolent. They may be benign follicular adenomas or they may be low risk differentiated thyroid cancers. So knowing that, we maybe more likely to observe the patients in certain cases or to just do a thyroid lobectomy. So Thyroseq V3 has that information, which I think is already in useful for prognosis and will be increasingly more so in the future. Now Affirma GSC has expression atlas, which has the potential to provide a lot of the similar type of information. But it is not yet clinically validated. So we don’t have a lot of data yet about how we use that for prognosis.
[Michael Yeh] Great. Thank you so much for sharing your insights with us today.
Got Questions About Indeterminate Thyroid Nodules?