2026 Research Day Program
Venue Information & Navigation
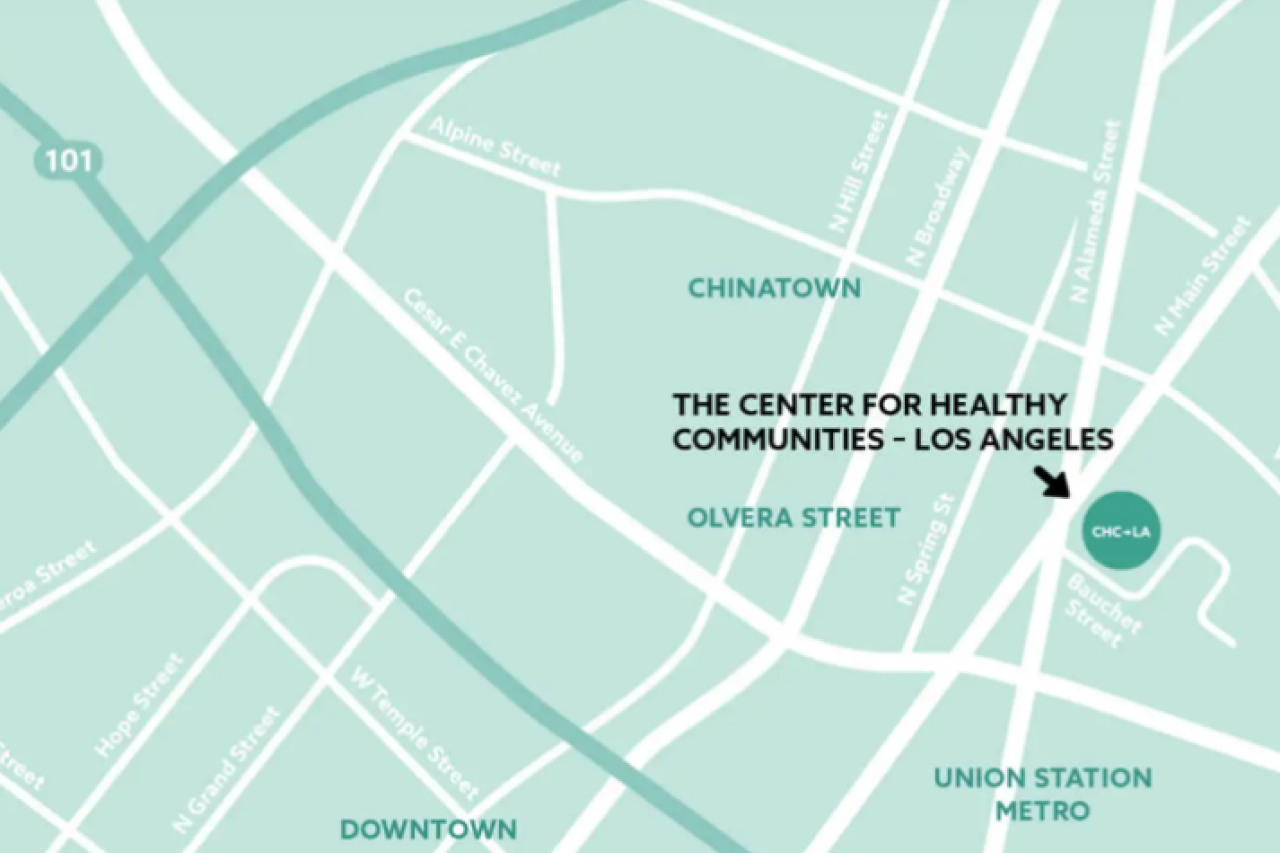
Directions to and Parking at the California Endowment
Research Day will be hosted at The California Endowment Center for Healthy Communities Los Angeles at . From Alameda St., turn onto Bauchet St. (stoplight) and continue to The California Endowment’s parking lot. We encourage attendees to carpool if possible. The venue is also easily accessible by public transportation, as it is within walking distance of the Union Station Metro. Free parking is available on a first-come, first-served basis. If the parking lot becomes full, we recommend you have cash as several nearby parking lots are cash-only.
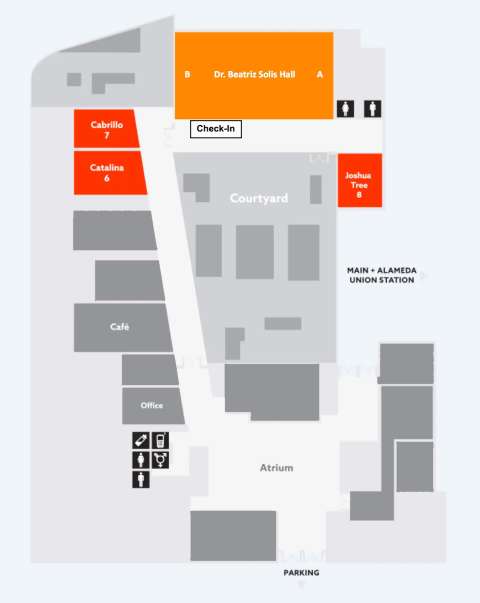
Map of Venue
Agenda
Faculty Development (Morning Session) (Invitation Only)
Time | Location | Event |
|---|---|---|
8:00AM – 8:30AM | Dr. Beatriz Solis Hall and Foyer | Check-In and Breakfast |
8:30AM – 9:15AM | Dr. Beatriz Solis Hall | Teaching Residents in the Era of AI - Dr. Thalia Nguyen (UCLA Clinical Informatics), Dr. Daniel Lee (UCLA APD), Dr. Anita Wong (UCLA APD) |
9:15AM – 9:45AM | Dr. Beatriz Solis Hall | Providing Medical Student Feedback - Dr. Olivia Ishibashi and Dr. Thalia Nguyen (UCLA FM Clerkship Chairs) |
9:45AM – 10:00AM | Dr. Beatriz Solis Hall and Foyer | Break |
10:00AM - 11:00AM | Dr. Beatriz Solis Hall | Clinical Reasoning Remediation - Dr. Matthew Yu (CDU PD) |
11:00AM - 11:30AM | Dr. Beatriz Solis Hall | Resident Practice Reports - Dr. Denise Sur (UCLA PD), Dr. Thalia Nguyen (UCLA Clinical Informatics) |
Research Day (Afternoon Session)
Time | Location | Event |
|---|---|---|
11:30AM – 12:00PM | Dr. Beatriz Solis Hall and Foyer | Research Day Check-in, Lunch, and Seating |
12:00PM – 12:05PM | Dr. Beatriz Solis Hall | Welcome and Introductions – by Gerardo Moreno, MD |
12:05PM – 12:55PM | Dr. Beatriz Solis Hall | Keynote: Carol M. Mangione, M.D., M.S.P.H. “US Preventive Task Force Guidelines: Updates, Methods, and Challenges for Addressing Health Equity” |
12:55PM – 1:00PM | Dr. Beatriz Solis Hall | Keynote Q&A |
1:00PM – 1:40PM | Cabrillo, Catalina, and Joshua Tree | Poster Session 1 At 1:15pm abstract presenters will provide a 60-second oral summary of their projects in each breakout room. Throughout the 40 min Poster Session, we encourage attendees to visit all three break-out rooms and ask questions of the authors. |
1:40PM – 2:25PM | Dr. Beatriz Solis Hall | Lectern Session 1 (Moderated by Dr. Bruno Lewin) |
2:25PM – 3:05PM | Cabrillo, Catalina, and Joshua Tree | Poster Session 2 At 2:40pm abstract presenters will provide a 60-second oral summary of their projects in each breakout room. Throughout the 40 min Poster Session, we encourage attendees to visit all three break-out rooms and ask questions of the authors. |
3:05PM – 3:50PM | Dr. Beatriz Solis Hall | Lectern Session 2 (Moderated by Dr. Parastou Farhadian) |
3:50PM – 4:00PM | Dr. Beatriz Solis Hall | Closing Remarks (Dr. Parastou Farhadian) and Raffle Winners Announced |
Keynote (12:00 - 1:00PM)
Speaker: Carol M. Mangione, MD, MSPH

Carol M. Mangione, M.D., M.S.P.H., is Chief of the Division of General Internal Medicine and Health Services Research and holds the Barbara A. Levey, MD, and Gerald S. Levey, MD, Endowed Chair in Medicine at the David Geffen School of Medicine at UCLA, where she also serves as Department of Medicine Executive Vice Chair for Health Equity and Health Services Research. She is also a Distinguished Professor of Public Health at the UCLA Fielding School of Public Health and directs the UCLA Resource Center for Minority Aging Research/Center for Health Innovation Maximizing Eldercare and the UCLA CTSI Workforce Development Program. A practicing primary care physician, her areas of expertise include development of preventive service recommendations, diabetes prevention, health disparities, aging, and health insurance benefit design. She is a member of the National Academy of Medicine, the American Society of Clinical Investigation, the American Diabetes Association, and several other leading professional societies. Dr. Mangione has led numerous federally funded research initiatives focused on diabetes prevention, medication adherence, and care innovation for underserved populations, with support from the CDC, NIDDK, and other agencies. She has authored more than 350 peer-reviewed articles and seven book chapters. A dedicated mentor, she was named an inaugural member of the UCLA Faculty Mentoring Society and received the 2022 Alan M. Fogelman Mentorship Award. She was appointed Chair of the U.S. Preventive Services Task Force in March 2022, having previously served as a member and vice chair. Dr. Mangione received her B.S. from the University of Michigan, her M.D. from UC San Francisco, and her M.S.P.H. from the Harvard School of Public Health, and completed fellowships at Harvard Medical School.
Keynote Address
Dr. Carole Mangione will be presenting on “US Preventive Task Force Guidelines: Updates, Methods, and Challenges for Addressing Health Equity” from 12:00pm - 1:00pm in the Dr. Beatriz Solis Hall. There will be a short Q&A following the keynote address.
Poster Session 1 (1:00 – 1:40PM)
Cabrillo Room - Abstracts
Immigration-Related Stress, Access Barriers, and Urgent Care Utilization: A Quantitative Survey
AUTHORS: Urania Argueta BA*, Daisy Hernandez-Casas BS*, Gerardo Moreno MD, MS, Ann Marie Hernandez MD, MPH
AFFILIATIONS: UCLA DGSOM PRIME-LA, COE
INTRODUCTION: Anti-immigrant rhetoric and enforcement actions have created a climate of fear deterring all immigrants from seeking care. This is compounded by California's Medi-Cal enrollment freeze for certain undocumented adults and the removal of safe haven protections for hospitals and schools. Historically, EDs and urgent care centers serve as safety-net access points for immigrants who delay care due to immigration-related fears or lack of primary care. We aim to examine associations between immigration-related stress, insurance status, delayed care-seeking, and comorbidities among patients across Los Angeles County clinics and urgent care centers.
METHODS: This cross-sectional survey study uses REDCap for data collection, with questions adapted from the California Health Interview Survey (CHIS), the Person-Centered Primary Care Measure, the KFF/New York Times 2025 Survey of Immigrants, and the UCSF SOIS. The study will be conducted at multiple Los Angeles County sites, including Mid-Valley Comprehensive Clinic urgent care, Clínica Romero, Mission Community Hospital Family Medicine Teaching Clinics, and Venice Family Clinic. Participants will be randomly sampled from waiting rooms and compensated with gift cards. Key exposures include self-reported immigration status and related stressors, patient-provider trust, primary language, and insurance status. Outcomes include comorbidity burden and urgent care utilization patterns.
RESULTS: We expect a majority of non-citizen participants will report delayed care-seeking behaviors. Most participants with a high number of urgent care visits will have a high disease burden in terms of the number of comorbidities and the severity of disease.
CONCLUSIONS: Findings from this study will raise awareness of the direct impact of immigration raids and changes to Medi-Cal coverage on immigrant communities in Los Angeles County. Survey findings may inform policy and advocacy initiatives to reduce healthcare utilization costs by improving access to care and reducing barriers to timely care-seeking.
Insurance Without Access: Primary Care Gaps and Unmet Specialty Needs Among Patients Experiencing Homelessness at a Free Clinic
AUTHORS: Gladys Bello, BS; Jacqueline Cabral, BA; Alejandra Rivas, BA; Joselyne Camacho, BA; Leonor Georgette Farias, BS; Selin Lopez, BA; Jyoti Puvvula, MD, MPH; Gilberto Granados, MD, MPH
AFFILIATIONS: UCLA PRIME, Harbor-UCLA Medical Center Department of Family Medicine
INTRODUCTION: Health insurance is necessary but often insufficient for access to care among persons experiencing homelessness. Free clinics have traditionally served uninsured populations, yet see increasing numbers of insured patients, suggesting persistent barriers to primary care. The Redondo Beach Free Clinic (RBFC), operated by Harbor-UCLA Family Medicine, serves a predominantly unsheltered population in Los Angeles County. UCLA PRIME-LA medical students partner with the RBFC, to address gaps in care. We conducted a needs assessment to describe the relationship between insurance status and actual access to care in this population.
METHODS: Survey data were cleaned and analyzed using R (version 4.5.2). Descriptive statistics were calculated after recoding insurance status into a binary variable (insured vs. uninsured), with missing responses excluded from denominators. We performed a cross-sectional analysis of needs assessment data collected at RBFC from March 2023 through October 2024 (N = 46). Variables included demographics, housing status, insurance coverage, primary care provider status, healthcare use in the previous six months, mental health conditions, and self-reported assistance needs. Descriptive statistics were used to summarize sample characteristics and access to care.
RESULTS: Among participants who reported insurance status (n=43), 74% (n=32) had health insurance. Insured participants who responded to the primary care question (n=30), 53.3% reported not having an established primary care clinician. Access barriers extended beyond primary care: among insured participants, 70.0% reported no dental visit, and 75.9% reported no vision visit within the prior six months. Participants were predominantly male (72%, n=33), unemployed (85%, n = 37), and unsheltered (57%, n=24). Mental health burden was high, with 51% reporting anxiety or depression; but, only one participant explicitly requested mental health services. Patient-identified priorities included housing (71%, n=30), dental care (67%, n = 28), transportation (57%, n=24), and food access (55%).
CONCLUSIONS: Insurance coverage did not translate into access to care among patients experiencing homelessness. Over half of insured participants lacked a primary care clinician, and most were unable to access dental or vision services. These findings highlight persistent structural barriers, including housing instability and transportation. In response, UCLA PRIME-LA partnered with UCLA Luskin MSW students to implement monthly patient navigation at RBFC, supporting care linkage and referrals. Integrating navigation services may improve continuity of care and inform future safety-net interventions.
Predictors of Musculoskeletal Pain and Pain Management Among Migrant Farmworkers From Oxnard, California
AUTHORS: Diego Cisneros (1,2), Jose Segura-Bermudez (1), Wendy Perez (1,2), Leslie Nunez (1,2), Alejandra Rivas Deras (1,2), Monica Soto Noveron (1,2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA; (2) La Cosecha Community Health Education Chairs
INTRODUCTION: Musculoskeletal (MSK) pain is a leading cause of disability around the world, disproportionately burdening migrant farmworkers due to physically demanding tasks, systemic barriers, and language exclusion. While physical demands are documented, the intersection of psychosocial stress and structural obstacles in migrant farmworking communities remains poorly understood. This study characterizes MSK pain burdens and predictors in Oxnard, California, while identifying cultural beliefs and critical gaps in injury prevention and pain management. The purpose of this study is to provide a foundation for a targeted health education curriculum.
METHODS: This cross-sectional study assesses MSK pain and beliefs using the adapted Nordic Musculoskeletal Questionnaire, Migrant Farmworker Stress Inventory, and California Agricultural Worker Health Survey. The survey was administered in English and Spanish and was written at a 6th grade level. 65 participants were recruited as a convenience sample at a health fair in Oxnard, California. Inclusion required farmwork within the past year. Primary outcomes were region-specific pain over 12 months, pain interference with work, and pain management sources. Predictors include type of agricultural work, years in fieldwork, insurance status, and psychosocial domains. Secondary predictors include healthcare access and immigration-related fears. Data was analyzed using descriptive and univariate methods.
RESULTS: Of the 65 farmworkers surveyed (92% Mexican-born, 64% female, mean age 43, 16 years in agriculture), 92% reported MSK pain in the past 12 months. The most affected regions were the lower back (52.3%) and upper back (40%). Most were pickers (84.6%) who sought clinic care (76.9%). Treatments included acetaminophen (47.7%), ibuprofen (46.2%), and herbal remedies (38.5%). Pain interfered with work for 59% and reduced income for 47%. Cost, immigration concerns, psychosocial stress, and injury reporting fears were significantly associated with both work interference and lost income (p<0.05). Desired interventions included stretching (67.7%), mechanics education (46.2%), low-cost care, and language-concordant information.
CONCLUSIONS: This study demonstrates a high burden of MSK pain among migrant farmworkers, with significant functional and economic impacts. The findings suggest that beyond physical labor, psychosocial stressors and immigration-related fears are key predictors of pain work interference and lost income. Future interventions should prioritize low-cost, language-concordant care and culturally tailored injury prevention. Addressing these structural and emotional barriers is essential for improving occupational health outcomes and economic stability in this vulnerable population.
Informing Patient-Centered Diabetes Care: Communication Preferences About GLP-1 Receptor Agonists
AUTHORS: Lucia Diaz (1), Dr. Ann Hernandez, MD, MS, MPH (2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA; (2) Department of Family Medicine at UCLA
INTRODUCTION: Latinos have higher prevalence of type 2 diabetes and complications yet are less likely to be prescribed GLP-1 receptor agonists (GLP1ra) compared to non-Hispanic white patients. GLP1ra improve glycemic control and have additional benefits such as weight loss, renal protective effects, and cardiovascular risk reduction. Limited English proficiency (LEP) is associated with poorer health status due to being unable to understand important health information. Given these intersecting challenges, it is imperative to understand how LEP Latinos with T2DM receive and prefer to learn information about newer diabetes medications like GLP1ra.
METHODS: This study will use qualitative methods and semi-structured 1-on-1 interviews. The interviews will be audio recorded, professionally transcribed, and translated to English. The interview guide was developed using existing literature and the health belief model approach.
Study participants will be recruited from UCLA clinics and included Spanish speaking older Latino adults (>60 yo) with T2DM. The interviews will be transcribed and analyzed to identify thematic codes. Our analytical approach will use thematic analysis which entails identifying emergent themes during the examination of participant interviews and subsequently organizes these themes into cohesive clusters and central concepts. Participants will be compensated with a $25 gift card.
RESULTS: The findings will identify the extent to which current approaches align with patient preferences to clarify where breakdowns in communication occur and highlight opportunities to improve engagement. Additionally, digital health engagement will be characterized including the use of patient portals, telehealth, and electronic messaging to determine the impact it has on a patient's ability to meaningfully participate in discussions about GLP1ra. The role of caregivers and family influence on patient understanding of medication risk and benefits and willingness to initiate GLP1ra will also be identified. It is expected to identify patterns in which caregiver engagement serves as a facilitator of shared decision making.
CONCLUSIONS: This project fills gaps in the literature regarding the use of GLP1ra in Latino communities and informs how to create culturally tailored approaches to patient education, medication adherence, and shared decision making in Spanish. Modifiable barriers to prescribing GLP1ra will be identified, allowing clinicians to incorporate structured approaches such as involving family members in counseling and potentially integrating digital health tools into routine care. This project will facilitate equitable diabetes care by ascertaining how to optimize the delivery of evidence-based therapies.
Artificial Stone Associated Silicosis Registry: A Study Protocol for Prospective Data Collection in Artificial Stone-Exposed Workers
AUTHORS: Nancy Gutierrez, MPH (1), Nitin Agrawal, MD (3), Nicolas Baddour, MD (3), Hector Rivera Marero, MD (5), Darlene Castro (2), Michelle Wan, MD (4), Shephali Gandhi, MD, MPH (5,6), Jane C. Fazio, MD, PhD (1,3)
AFFILIATIONS: (1) David Geffen School of Medicine, University of California, Los Angeles, Los Angeles CA; (2) Education and Research Institute Olive View UCLA Medical Center, Sylmar CA; (3) Department of Medicine, Division of Pulmonary, Critical Care and Sleep Medicine, University of California Los Angeles, Los Angeles CA; (4) Department of Medicine, Olive View UCLA Medical Center, Sylmar CA; (5) Division of Occupational, Environmental, and Climate Medicine, University of California San Francisco, San Francisco; (6) Division of Pulmonary, Critical Care, Allergy, and Sleep Medicine, University of California San Francisco, San Francisco
INTRODUCTION: Silicosis is a fibrotic occupational lung disease caused by chronic inhalation of respirable crystalline silica, with lung transplantation as the only definitive therapy. Workers who fabricate artificial stone (AS) countertops, in California primarily Latino immigrants, have been identified as high risk for development of silicosis. The purpose of this study is to first, clarify the natural history of AS silicosis. Second, to create a biorepository to support translational research on disease mechanisms and progression including biomarker identification. To do this we will establish a longitudinal, observational cohort of AS-exposed workers.
METHODS: AS-exposed workers with and without silicosis will be recruited at their routine clinical appointments at the UCLA Olive View Pulmonary Clinic or the UCSF Occupational and Environmental Medicine Clinic. At baseline and at least every 12 months, participants will complete the occupational and symptom questionnaire, the King's Brief Interstitial Lung Disease questionnaire, the Modified Medical Research Council Dyspnea Scale, and the Patient-Reported Outcomes Measurement Information System. Clinical data includes pulmonary function testing, six-minute walk distance, chest CT, pathology, laboratory data, microbiology, echocardiogram and right heart catheterization data. We will also collect blood samples and nasopharyngeal swabs for biobanking and use in identification of biomarkers.
RESULTS: Preliminary results include questionnaires from 26 participants enrolled between September 2025 and February 2026 at UCLA. All were Latino men from Mexico or Central America, with a median age of 51 years and varied immigration statuses, including 46% undocumented. They reported worse-than-average outcomes in physical function, anxiety, depression, and fatigue. At least half reported worrying about lung disease severity, anticipating worsening symptoms, and thinking about the end of life. Over half (55%) had mMRC score greater than or equal to 2, indicating significant dyspnea. Only 35% had full-scope health insurance. 23% used no respiratory protection, 31% used surgical masks, and 77% used an N95, none of which meet current safety standards.
CONCLUSIONS: Despite ongoing efforts to reduce workplace exposure to respirable silica, we expect to continue to see a rise in patients with silicosis. A clearer understanding of the disease mechanism will aid in the development of targeted therapies to slow down, or completely stop, disease progression. This registry will enable characterization of disease trajectories, symptom burden, and functional decline over time, and will support hypothesis generation for future clinical and translational studies of this emerging occupational lung disease.
Identifying Barriers to Food, Shelter, and Primary Care Through a Community-Engaged Street Medicine Initiative
AUTHORS: Abigail Hendrie, BS (1), Gerardo Moreno, MD, MS (2), Mary Marfisee, MD, MPH (2)
AFFILIATIONS: (1) David Geffen School of Medicine, University of California, Los Angeles; (2) Department of Family Medicine, University of California, Los Angeles
INTRODUCTION: Unhoused populations face disproportionately high burdens of chronic disease, food insecurity, and barriers to primary care. Studies show high rates of malnutrition, psychiatric illness, substance use disorders, and inconsistent healthcare and nutrition access [1-4]. Despite a growing unhoused population in Westwood Village, key service gaps remain. Most live in isolation and lack access to consistent nutrition, primary care, and housing resources. To address this gap, we developed and implemented a student-led street medicine initiative to understand key needs and provide hot meals, medical care, and connection to social services.
METHODS: We partnered with a local organization to conduct initial outreach and establish rapport. Then, we implemented weekly street medicine rounds with the UCLA Student-Run Homeless Clinic over twelve months. We provided hot meals, medical care, and assistance with social services. Semi-structured qualitative interviews, clinical observation, and surveys were used to assess housing, food insecurity, primary care access, medical conditions, demographics, and basic needs. The study included 77 individuals, representing nearly the entire Westwood Village unhoused population. Data was analyzed to identify recurrent needs, chronic conditions, and barriers to care. Thematic saturation was achieved after encounters demonstrated consistent patterns of unmet need and disease burden.
RESULTS: 78% were solitary men, most commonly aged 40-50. Key unmet needs included shelter, food, primary care, mental health services, and basic resources. Many reported difficulty finding shelter following hospital discharge or incarceration, with barriers including long waitlists, limited social worker access, and lack of phones. None identified a reliable source of free hot meals; most relied on informal sources or government assistance. Chronic medical conditions were common and poorly managed, with inconsistent primary care, low medication use, and limited engagement in health behaviors. Barriers included geographic inaccessibility, competing survival priorities, and medication storage concerns. A centralized Westwood location for medical care, hot meals, and case management is needed.
CONCLUSIONS: Continuity and consistent outreach through hot meals were key to establishing rapport with this community, gaining the trust necessary to initiate complex healthcare and housing navigation. This population faces profound, interconnected barriers, including severe food insecurity, housing instability, and very limited access to primary care. These challenges perpetuate unmet needs and untreated health conditions, reinforcing barriers to care. Community-based street medicine outreach can address immediate needs while building trust and connecting individuals to housing and healthcare services.
Psychosocial factors associated with methamphetamine use in men receiving a smartphone cognitive behavioral therapy intervention for reducing methamphetamine use and HIV risk behaviors
AUTHORS: Christopher Mason; Michael Li, PhD; Chunqing Lin, PhD; Cathy Reback, PhD
AFFILIATIONS: University of California, Los Angeles
INTRODUCTION: Methamphetamine (MA) use is associated with increased HIV risk behaviors among men who have sex with men (MSM) and poor HIV treatment outcomes in MSM living with HIV. The Getting Off app, a smartphone-based cognitive behavioral therapy intervention for MSM, has been shown to reduce MA use and some sexual risk behaviors, but it is unknown whether certain psychosocial factors were associated with augmented or attenuated treatment response.
METHODS: The present study is a longitudinal secondary data analysis of participants in the Getting Off app randomized controlled trial. Psychosocial factors of interest included repeated measures of self-reported depressive symptoms, housing instability, and income over 9 months. Outcomes included repeated measures of number of days of MA use in the past 30 days, number of days of MA injection in the past 30 days, and CAI, CAI while using MA, all evaluated over 9 months. Mixed effects negative binomial regressions and mixed effects logistic regressions were used to evaluate associations between psychosocial factors and these outcomes.
RESULTS: Participants with depressive symptoms had 47% more days of MA use in the past 30 days (IRR 1.47, 95% CI [1.18, 1.83], p < 0.001) and 3.20-fold greater odds of CAI while using MA (OR 3.20, 95% CI [1.67, 6.13], p < 0.001). They also had higher baseline odds of any CAI (OR 3.65, 95% CI [1.95, 6.82], p < 0.001) but showed a 14% greater monthly reduction in CAI (OR 0.86, 95% CI [0.77, 0.96], p = 0.008). Income >=$15,000 was associated with 35% fewer days of MA use in the past 30 days (IRR 0.65, p = 0.018) and 64% fewer days of MA injection in the past 30 days (IRR 0.36, p = 0.032), but higher odds of CAI (OR 3.37, p = 0.004) and CAI while using MA (OR 2.90, p = 0.014). Homelessness was not associated with outcomes. Time was associated with reductions in MA use, injection, and CAI while using MA.
CONCLUSIONS: Depressive symptoms were associated with greater MA use and CAI, while income showed mixed associations, highlighting the added importance of addressing of other contextual factors in smartphone-based behavioral interventions.
Language Barriers and Inequities in Diabetes Care: Evidence to Inform Policy Solutions for Equitable Access in California
AUTHORS: Leslie Nuñez, BS (1), Alejandra Rivas Deras, BA (1) Beza Mengistu, BS (1), Ann Marie Hernandez, MD, MPH, MS (2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA , (2) Department of Family Medicine at UCLA
INTRODUCTION: In 2021, 38.4 million people in the U.S. had diabetes, accounting for 11.6% of the U.S. population.1 Diabetes is the eighth leading cause of mortality in the U.S. and remains a significant cause of disability and decreased quality of life.2 Historically marginalized groups bear a disproportionate burden of diabetes and its associated complications.3 Limited English proficiency (LEP) represents a critical yet underexamined determinant of diabetes care. This study examines disparities in diabetes care processes, access to care, and use of health services among individuals with LEP using data from the California Health Interview Survey (CHIS).
METHODS: This cross-sectional study used data from the 2024 California Health Interview Survey (CHIS) to examine disparities in diabetes care, access, and healthcare utilization among adults with limited English proficiency (LEP), defined as speaking English less than “very well,” compared with English-proficient (EP) adults. Adults (≥18 years) with self-reported diabetes were included. Outcomes included receipt of hemoglobin A1c testing, dilated eye exams, and a diabetes care plan. Measures of access and utilization included having a usual source of care, difficulty understanding a physician, receipt of telehealth services, and delays in obtaining prescribed medications. Descriptive statistics were used to summarize sociodemographic characteristics and contextualize the study population.
RESULTS: Of 1,357 respondents, 1,017 (75%) were EP and 340 (25%) were LEP. HbA1c testing varied modestly, with more LEP respondents reporting no testing in the past year (14% vs 6.6%, p < 0.001 ). EP adults were more likely to report a dilated eye exam within the last 2 months, while LEP adults more often reported no or less recent exams. Receipt of a diabetes care plan was higher among EP individuals (83% vs 70%, p < 0.001). Having a usual source of care was more common among EP adults (93% vs 84%, p < 0.001). LEP respondents more frequently reported difficulty understanding a physician (9.7% vs 5.3%, p = 0.023). Telehealth use was higher in EP adults (47% vs 30%, p < 0.001) and among insured participants, delayed or missed medications were more common among EP individuals (73% vs 48%, p = 0.002).
CONCLUSIONS: Results of this study demonstrate that LEP adults with diabetes experience consistent disparities in care processes and access and utilization of services compared with their EP counterparts. Lower rates of recommended monitoring and reduced access to a usual source of care suggest gaps in system-level language access. These findings support strengthening use of interpreter services, expanding culturally and linguistically appropriate diabetes care programs, and integrating language access metrics into quality improvement and health policy efforts.
Managing MSK sequelae and pain in Cancer Survivors to improve function and Quality of Life
AUTHORS: Shivam Patel OMS-III; Jose Urbina MD; Amirpasha Ehsan MD; Harnek Singh MD
AFFILIATIONS: Western University COMP, Clinica Sierra Vista/Kern, Providence St. Jude
INTRODUCTION: With nearly 19 million cancer survivors in the United States, and an expected increase in cancer incidence and prevalence due to rising life expectancy, the growing number of long-term functional sequelae of cancer treatment is becoming a major public health concern. There are a variety of common MSK impairments following treatment of cancers which impact mobility, cause fatigue, contribute to deconditioning, and limit return to normal activities of daily living (DAL). Conventional approaches under-utilized rehabilitation services, with one case showing only roughly 30% of patients warranting rehab referral received it.
METHODS: Scholarly databases, such as PubMed, Google Scholar, MedlinePlus, Physiatry.org, the American Cancer Society (ACS), and the National Cancer Institute (NCI) educational portals were used. For additional information regarding clinical guidelines and criteria, the Commission on Cancer and American Academy of Physical Medicine and Rehabilitation were utilized. Key term searches included: cancer rehabilitation, prehabilitation, head and neck cancer rehabilitation, breast cancer functional disorders, PM&R in oncology, multimodal pain management in cancer survivorship, multidisciplinary survivorship care, occupational therapy, and physical therapy. Anonymized Information from one patient case was also used to review management.
RESULTS: Cancer treatments were found to cause a variety of musculoskeletal complications that significantly impair patients’ DAL. Collectively, these impairments contribute to chronic pain and diminished quality of life, making cancer survivors ideal candidates for rehabilitation intervention and multi-modal pain management which can be addressed by primary care physicians. Literature across cancer types demonstrates that early, individualized rehabilitation can interrupt this cycle of dysfunction. Targeted PT and exercise-based conditioning improves strength and endurance while decreasing pain. Addressing common MSK sequela following incidences of breast cancer, lymphoma, and other head/neck cancers, could prevent long-term disability and improve outcomes among cancer survivor populations.
CONCLUSIONS: Long-term functional sequela of cancer treatment, particularly the symptomatic burden on the MSK system, can be addressed with the incorporation of rehabilitation into traditional pain management approaches has shown to improve outcomes. Preemptive intervention, establishing a functional baseline, and following up with structured intervention can preserve independence and prevent further decline. Understanding the mechanisms behind dysfunction in cancer patients can aid primary care physicians in optimally managing common MSK sequela that cancer survivors presenting with in outpatient settings.
Adaptation of Contingency Management to Facilitate Retention in Supportive Housing: A Pilot Evaluation Study
AUTHORS: Allison D. Rosen, PhD (1), Aarushi Saharan, BS (1), Grace Yi, MSPH (1), Omar Nieto, BA (1), Denise Guzman-Naranjo, BS (1), Joshua Florence, BS (1), Shoshanna Scholar, BS (2), Anna Gorman, MPH (2), Jessica Reyes, MPH (2), Daniel Bonilla, MPH (2), Carlton Rucker, MEd (3), Allyza Quintanilla, BS (3), Steven J. Shoptaw, PhD (1)
AFFILIATIONS: (1) Department of Family Medicine, David Geffen School of Medicine, University of California Los Angeles, Los Angeles, CA; (2) Los Angeles County Department of Health Services, Los Angeles, CA; (3) The People Concern, Los Angeles, CA
INTRODUCTION: Substance use and resulting disruptive behaviors are common causes of eviction from supportive housing. Contingency management (CM), which uses increasingly valuable incentives to reward positive behaviors, was developed for use in adolescent group homes and is a first-line treatment for stimulant use disorder. Building on this evidence base, this study adapted CM for residents of supportive housing with a history of substance use, hypothesizing that participation in the adapted CM program would be associated with reduced disruptive behaviors and increased likelihood of housing retention.
METHODS: This mixed methods study was conducted at six permanent supportive (PSH) and four interim (IH) housing sites in LA County, enrolling 139 residents with history of substance use or disruptive behaviors. Participants set a goal to reduce a behavior that was impacting their housing stability. At twice weekly meetings for 12 weeks, evidence of behavior change was rewarded with gift cards. The primary outcomes, percentage of meetings where participants demonstrated reduced disruptive behaviors and percentage housed at 12 weeks, were compared for PSH and IH participants. Modified Poisson regression tested the association of decreased disruptive behavior and housing status at 12 weeks. Participant perspectives were assessed using coding reliability thematic analysis of 32 in-depth interviews.
RESULTS: Of 139 enrolled, 65% lived in PSH and 35% in IH. Over 75% were aged 30-59 and 40% identified as women, 51% as men, and 9% as transgender; 43% identified as Black, 28% Hispanic, 22% white, and 7% other. The median percentage of meetings with reduction in disruptive behavior was 58% (IQR: 33-75%) in PSH and 29% (IQR: 4-46%) in IH (P<0.001). At 12 weeks, 83% from PSH and 47% from IH remained housed (P<0.001). For each 10% increase in meetings where reduced disruptive behavior was demonstrated, likelihood of remaining housed was the same in PSH (aRR: 1.02, 95% CI: 0.98-1.07, P=0.28), but increased by 18% (aRR: 1.18, 95% CI: 1.08-1.29, P<0.001) in IH. Interview participants said the program helped them connect behaviors to housing stability and motivated them to make positive changes.
CONCLUSIONS: Findings from this study suggest that an adapted CM program is a promising intervention for reducing disruptive behaviors that lead to eviction from supportive housing. Future iterations could further adapt this methodology to the unique settings of PSH and IH where tolerance of disruptive behaviors and threshold for eviction differ. Future work should also include a control group to better understand trajectories of disruptive behaviors and housing retention for residents who do not receive the adapted CM intervention.
Improving Pathology Communication: A PDSA-Based Pilot of Patient-Centered Educational Tool
AUTHORS: Laura Solano, BS (1); Somtochukwu Uzoka, BS (2); Michele Mitchell, BS, MS, PMP (3); Kenechukwu Ojukwu, MD, MS, MPP (4)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA, Los Angeles, CA; (2) California State University, Northridge, CA; (3) American Society for Clinical Pathology; (4) UCLA Department of Pathology and Laboratory Medicine
INTRODUCTION: Clear communication of pathology cancer diagnoses directly impacts health literacy and patient outcomes. With input from primary care, dermatopathology, and patient advocates, we designed a brochure to enhance skin cancer diagnostic communication in primary care settings. We will survey primary care physicians to assess acceptability, usability, feasibility, and adoption as part of a formative evaluation. Pilot testing of the survey with medical students provided an opportunity for iterative refinement using a Plan-Do-Study-Act (PDSA) framework, centering early stakeholder-informed design.
METHODS: We conducted a multi-phase quality improvement pilot using a Plan-Do-Study-Act (PDSA) framework. A structured REDCap survey was administered to 57 medical students (MS1–MS4) over 5 days following review of a patient-centered pathology education brochure. Outcomes included confidence in communicating pathology results, perceived adequacy of training, and tool usability. Likert responses were summarized using medians/IQR and descriptive statistics; subgroup comparisons were performed using independent t-tests. Open-ended responses underwent thematic analysis to identify barriers and inform iterative refinement prior to evaluation among primary care providers.
RESULTS: Baseline preparedness for pathology communication was low, including confidence in discussing results with patients (2 [IQR 1–2]) and perceived training adequacy (2 [2–3]). Confidence increased with training level (MS1 1.47 vs MS2+ 2.08, p=0.009) but remained limited. Prior dermatology/pathology exposure trended toward higher confidence (2.33 vs 1.75, p≈0.055). The brochure received high ratings for usability and communication value (mean ~4.1/5), including navigation (4.18) and patient-centered communication (4.22).
Qualitative findings showed key themes including readability, patient empowerment, and workflow integration. Students valued clear, jargon-free explanations and the “Questions to Ask” section, and recommended improved visuals and digital integration (e.g., QR-linked content).
CONCLUSIONS: Trainees demonstrate low preparedness for pathology communication, while a patient-centered educational tool shows high acceptability and potential to support clinical discussions. These findings highlight a critical gap in communication training and suggest that simple, scalable interventions may improve patient understanding in primary care settings. Ongoing work will expand evaluation to primary care providers and assess implementation barriers to using the tool in clinical practice, including workflow integration and real-world adoption within primary care settings.
Identifying and Addressing Barriers to Pediatric Primary Care for Homeless Children in Los Angeles: A Community-Engaged Needs Assessment
AUTHORS: Rashna Soonavala (1), Mary Marfisee, MD, MPH (2)
AFFILIATIONS: (1) UCLA David Geffen School of Medicine; (2) Department of Family Medicine at UCLA
INTRODUCTION: Children experiencing homelessness face structural and informational barriers that limit access to pediatric care. These barriers manifest in delayed vaccinations, poorly controlled acute illnesses, unmanaged chronic conditions, and increased prevalence of developmental delay and severe autism, compared to the general population. At a Skid Row shelter serving approximately 75 families, only 1 in 4 families reported having health insurance and an established pediatric provider at a recent town hall. This study aimed to identify barriers to pediatric care and inform targeted, community-responsive solutions.
METHODS: This IRB-exempt qualitative study was conducted at a homeless shelter in Skid Row and through onsite visits in the surrounding community. Semi-structured interviews were performed with parents, shelter staff, social workers, local school nurses, a LAUSD Homeless Students Liaison, a family specialist, and childcare providers serving children experiencing homelessness. Interviews explored barriers to pediatric care, access to preventive services, and opportunities for supportive solutions. Interviews were conducted with verbal consent, de-identified, and analyzed using thematic analysis. Findings informed the development of targeted solutions.
RESULTS: A total of 24 interviews were conducted, including 16 families and 8 community stakeholders, representing approximately 20% of families in the shelter. Key barriers included insurance challenges (e.g., difficulty transferring benefits), limited awareness of resources, lack of documentation, legal status concerns, and competing priorities. Key solution areas included: (1) immediate insurance enrollment to facilitate reconnection to services such as Medi-Cal, (2) on-site pediatric care, and (3) improved navigation of community resources. Immediate actions included creation and distribution of an updated resource guide and organizational tools, as well as referral to local clinics for immunization updates.
CONCLUSIONS: Our study corroborated that children experiencing homelessness face barriers that limit access to care. Frequent community-engaged needs assessments are essential for identifying gaps and informing practical, low-cost solutions, including immediate insurance enrollment, on-site pediatric care, and close navigation of available resources. These findings support targeted approaches to improve care access and delivery for underserved children and families in life-altering housing instability.
Optimizing Resident Medical Education: Semantic Neighborhood Performance as a Predictor of Recall in Spaced Repetition Learning
AUTHORS: Gokul Sninivasan BS (1), Neha Srinivasan (2), Lucas Karamanoukian (3), Manuel Mendoza MD (4)
AFFILIATIONS: (1) David Geffen School of Medicine; (2) Dartmouth College; (3) Brentwood High School; (4) Department of Family Medicine, UCLA Health Toluca Lake
INTRODUCTION: Medical trainees must retain thousands of interconnected facts while caring for patients in real time. Spaced repetition platforms support active recall, but most recall prediction methods rely on a card's own review history and may miss concept-level signals when learners struggle with semantically related material. Using data from a real-world AI-enhanced medical spaced repetition platform, we evaluated whether performance on semantically neighboring cards predicts future recall beyond a card's own review history.
METHODS: We analyzed de-identified Anki review logs from a large medical deck. After deduplicating overlapping accounts, histories were transformed into one row per review. Note text was normalized and embedded. For each review, we identified the five most semantically similar notes among cards previously reviewed by that learner. Neighborhood performance was the pass rate on the neighbors' most recent reviews. Recall was defined as ease >=2. We measured the point-biserial correlation between neighborhood pass rate and recall, then trained two neural networks using chronological train/validation/test splits: card-history only versus card-history plus neighborhood features. Card-history features included prior ease, intervals, response times, and review timing.
RESULTS: Of 2,848,469 review events, 2,847,008 were analyzable, representing 43 learners and 467,578 learner-card pairs. Neighborhood performance correlated with current recall (k=5: r=0.4686, p<0.001). Current pass rate increased from 22.2% when neighborhood pass rate was 0-20% to 85.6% when it was 80-100%. The association persisted within learners (r=0.3559) and was strongest for cards with 0-2 prior reviews (r=0.5930). A card-history-only neural network achieved AUC/log loss/Brier score of 0.871/0.404/0.127; adding neighborhood features improved performance to 0.891/0.331/0.100. The largest gain was for first reviews, where AUC improved from 0.500 to 0.915.
CONCLUSIONS: Semantic-neighborhood performance predicted recall beyond card-specific review history, with the greatest benefit for first and early reviews. These findings suggest that concept-level signals may help spaced repetition platforms better personalize early knowledge reinforcement for medical learners. Content-aware scheduling may improve recall prediction while preserving card-specific scheduling for more mature material.
Medicaid Policy Changes and Immigration Enforcement: Impacts on Healthcare Access, Delivery and Clinician Experience in Los Angeles County Safety-Net Clinics
AUTHORS: *Lilia Diaz (1), *George Heredia (1), *Diana Jimenez-Briseno (1), *Dorian Kariuki (1), *Iman Kazah (1), *Makaelah Murray (1), Don Garcia, MD (3), Arthur Ohannessian, MD (4), Parastou Farhadian, MD (5), Cesar Barba, MD (6), Gerardo Moreno, MD, MS (1,2), Anne M. Hernandez MD, MPH (1,2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA; (2) Department of Family Medicine at UCLA; (3) Clínica Monseñor Oscar A. Romero, Los Angeles, CA; (4) Mid Valley Health Center, LAC DHS, Los Angeles, CA; (5) Mission Community Hospital, Panorama City, CA; (6)Venice Family Clinic, Venice, CA. *These authors contributed equally to this work
INTRODUCTION: Recent federal Medicaid policy changes under H.R.1 may reduce safety-net financing and disproportionately affect low-income, uninsured, and undocumented populations. Prior Medicaid funding reductions have been linked to decreased access, reduced services, and strained clinic capacity. Simultaneously, heightened immigration enforcement may further deter healthcare utilization. This clinician-focused arm of a coordinated three-pronged mixed-methods study examines patient and stakeholder understanding and experience while assessing early shifts in care access and outcomes at Los Angeles safety-net clinics.
METHODS: This current study aims to understand perspectives from clinicians, including residents and attendings, practicing in Los Angeles County safety-net clinics. In partnership with four community health centers across Los Angeles, semi-structured individual and group interviews were conducted with clinicians, including residents and attending physicians, to explore their understanding of the H.R.1-related policy changes, immigration enforcement, and experiences delivering care. Data is being analyzed using thematic analysis to identify emerging patterns and shared experiences.
RESULTS: Data collection and analysis are ongoing. Preliminary review of the first 18 clinician semi-structured interviews reflect broad themes related to concerns such as providing holistic continuity of care and access for underserved patient populations. Clinicians also described observations of immigration-related fear affecting healthcare utilization, increased psychosocial and financial stressors among patients and uncertainty surrounding insurance coverage and eligibility changes. Early interviews additionally reflect concerns on potential delays in preventive and chronic disease care. These findings are preliminary and exploratory, and formal thematic qualitative analysis is currently underway.
CONCLUSIONS: As safety-net clinics navigate pressures from Medicaid restructuring and immigration enforcement, understanding their intersecting effects on vulnerable populations is urgent. The approach captures system-level trends and lived experiences often absent from policy discussions. Findings intend to inform clinic-level adaptations and provide evidence to advocate for policy safeguards that protect equitable access for underserved communities in Los Angeles and beyond.
Medicaid Policy Changes and Immigration Enforcement: Impacts on Healthcare Access, Delivery and Patient Experience in Los Angeles County Safety-Net Clinics from the Administrators’ Perspective
AUTHORS: *Lilia Diaz (1), *George Heredia (1), *Diana Jimenez-Briseno (1), *Dorian Kariuki (1), *Iman Kazah (1), *Makaelah Murray (1), Don Garcia, MD (3), Arthur Ohannessian, MD (4), Parastou Farhadian MD (5), Cesar Barba, MD (6), Gerardo Moreno, MD, MS (1,2), Anne M. Hernandez MD, MPH (1,2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA; (2) Department of Family Medicine at UCLA; (3) Clínica Monseñor Oscar A. Romero, Los Angeles, CA; (4) Mid Valley Health Center, LAC DHS, Los Angeles, CA; (5) Mission Community Hospital, Panorama City, CA ; (6) Venice Family Clinic, Venice, CA. *These authors contributed equally to this work.
INTRODUCTION: Recent federal Medicaid policy changes under H.R.1, also referred to as the One Big Beautiful Bill, may reduce safety-net financing and disproportionately affect low-income, uninsured, and undocumented populations. Prior Medicaid funding reductions have been linked to decreased access, reduced services, and strained clinic capacity. Simultaneously, heightened immigration enforcement may further deter healthcare utilization. This qualitative study examines clinic administrators’ perspectives on the impact of H.R. 1 and assesses plans to mitigate anticipated shifts in care access and healthcare outcomes at Los Angeles safety-net clinics.
METHODS: The current administrative study stems from a larger study that includes patients and clinicians across four safety-net community clinics within Los Angeles. This study seeks to use semi-structured interviews to explore clinic administrators’ understanding of the effects of HR1-related policy changes and immigration enforcement on the accessibility and delivery of care. The interviews were audio taped and transcribed, and thematic analysis is ongoing. The Anderson-Gelberg theoretical Behavioral Model for Vulnerable Populations will serve as a guide for analysis and the dissemination of results.
RESULTS: To date, over twenty total interviews have been conducted across the three study groups, including five administrators from various safety-net clinics. Preliminary themes that have emerged from these interviews include varying policy awareness, how immigration enforcement will continue to impact clinic operations, and the financial risk and operational strain secondary to HR1’s implementation.
CONCLUSIONS: As safety-net clinics navigate pressures from Medicaid restructuring and immigration enforcement, understanding the intersecting effects of these policies on vulnerable populations is urgent. This study's mixed-methods approach will capture both system-level trends and the lived experiences often absent from policy discussions. Findings intend to inform clinic-level adaptations and provide evidence to advocate for policy safeguards that protect equitable access for underserved communities in Los Angeles and beyond.
Cabrillo Room - Case Reports
Postpartum Kidney and Liver Injury: Don't Miss the Other Causes
AUTHORS: Angela Aguirre, MD, Alma Alejandra Cortez, MD, Jesse Cheung, MD, Mohamed Elsharkawy, MD
AFFILIATIONS: Pomona Valley Hospital Medical Center FMRP
INTRODUCTION: Systemic lupus erythematosus (SLE) is a chronic autoimmune disease with relapsing-remitting, multisystem involvement. Pregnancy and the postpartum period are critical for disease fluctuations due to hormonal, immunologic, and physiologic changes. Lupus flare risk rises in the first 3 to 6 months postpartum, driven by rapid hormonal withdrawal, immune rebound, and stressors like sleep loss and recovery after childbirth.
METHODS: A 24-year-old woman, 4 months postpartum, presented to the emergency department after her primary care provider found elevated liver enzymes. She had a 3-month history of nausea, vomiting, 30-pound unintentional weight loss, decreased appetite, and progressive, migratory musculoskeletal pain affecting both upper and lower extremities. She also noticed dark orange, frothy urine. Family history revealed SLE in a maternal cousin. Initial labs showed pancytopenia, transaminitis, and proteinuria. Autoimmune serologies were positive for systemic lupus erythematosus and Sjögren’s syndrome overlap. Renal biopsy confirmed lupus nephritis. Corticosteroid therapy was started leading to improved liver function, hematologic abnormalities, and appetite.
DISCUSSION: This case highlights the importance of early consideration of autoimmune causes in postpartum patients with nonspecific symptoms. Delayed recognition may cause significant morbidity, including irreversible renal and liver damage. Timely diagnosis and immunosuppressive therapy are vital to prevent end-organ injury and reduce mortality and improving outcomes with prompt intervention and specialist referral.
Case Report: Decompression Sickness Secondary to Patent Foramen Ovale in a Recreational Scuba Diver
AUTHORS: Reid M. McCabe, MD
AFFILIATIONS: Department of Family Medicine at UCLA
INTRODUCTION: Patent foramen ovale (PFO) is present in ~27% of the general population and confers a 5-fold increased risk of decompression sickness (DCS) by permitting paradoxical right-to-left shunting of venous gas emboli into the arterial circulation. PFO is not routinely screened for prior to recreational diving, and diagnosis often follows a DCS event. We present a 56-year-old male recreational diver who developed severe neurological and vestibular DCS secondary to a previously undiagnosed PFO, subsequently managed with hyperbaric oxygen therapy and percutaneous closure, contrary to guidelines.
METHODS: A 56-year-old male with no significant medical history presented with acute severe dizziness, imbalance, nausea, vomiting, and near-syncope after completing 16–18 dives over multiple days in Cozumel, Mexico, to depths of ~80 feet with up to four dives daily. All dives followed standard decompression protocols. Symptoms began while showering after his final dive. He also reported decreased right ear hearing, tinnitus, and bilateral lower extremity paresthesias. Examination revealed cutis marmorata on the abdomen. Venous ultrasound demonstrated spontaneous intravascular bubbles in transit. He underwent hyperbaric oxygen therapy over several days with improvement in neurological symptoms. Echocardiography with bubble contrast demonstrated right-to-left shunting through a PFO. At cardiology follow-up ten months later, intracardiac echocardiography revealed an aneurysmal interatrial septum with right-to-left shunting. Successful percutaneous PFO closure was performed after a discussion of risks and benefits.
DISCUSSION: This case highlights key features of PFO-associated DCS: neurological and vestibular symptoms after protocol-compliant dives, cutis marmorata, and persistent inner ear injury — all hallmarks of paradoxical arterial gas embolization. The aneurysmal septum further increased embolic risk. PFO prevalence reaches 97% in divers with unprovoked DCS. SCAI guidelines conditionally recommend against routine PFO closure in divers, citing absent RCT data, but acknowledge closure is reasonable when patients highly value the potential benefit. Here, high-grade shunting, aneurysmal septum, severe index DCS, and the patient's desire to continue diving supported closure. Clinicians should consider PFO evaluation in any diver with DCS after properly performed dives.
Catalina Room - Abstracts
“Health Equity Check-In”: A QI Project to Address Inequities and Improve Well-Being in the Inpatient Setting
AUTHORS: Nate Bohm-Levine*, Katherine Iannuzzelli*, Spencer McCaffrey (*=co-first authors)
AFFILIATIONS: UCLA Department of Family Medicine
INTRODUCTION: Family physicians are uniquely positioned to address health inequities. Not being able to fully address health inequities during the workday can contribute to physician burnout. The inpatient family medicine setting provides an ideal context to discuss health equity topics related to admitted patients. We adapted a pediatric framework to create a Family Medicine “Health Equity Check-In” for the UCLA FM inpatient teaching service. We conducted a quality improvement project with the goal of improving discussion of health equity topics during inpatient wards and increasing physician well-being.
METHODS: A “Health Equity Check-In” poster and protocol was created. We developed pre- and post-surveys to assess resident physician and faculty’s ability to address health equity issues within the inpatient setting, as well as questions regarding interpreter usage and physician well-being. We used descriptive and inferential statistics to analyze results.
RESULTS: While further data collection and analysis is ongoing, a total of 21 respondents replied to the pre-survey, and 13 to the post-survey. Preliminary results revealed a statistically significant increase in comfort identifying, discussing, and addressing health inequities (all P < 0.05) compared to before starting the check-in. 15 out of 21 (71%) said that they somewhat or strongly agreed that health inequities impacted wellbeing. 8 out of 13 (62%) respondents said the amount of time discussing health inequities increased since using the check-in. 8 out of 13 (62%) respondents said they somewhat or strongly agreed that the check-in decreased frustrations. Some barriers to implementation include increasing length of time on rounds, and variability in who initiates the discussion.
CONCLUSIONS: Discussing health equity topics on inpatient rounds provides a structured way to address inequities and improve physician well-being during family medicine inpatient wards. Quality improvement PDSA cycles remain ongoing.
Consequences, not quantity, as a screening tool for substance use disorder (SUD)
AUTHORS: Alison Butler, MD PhD, Gloria Sanchez, MD FASAM, Bernadette Pendergraph, MD
AFFILIATIONS: Department of Family Medicine, Harbor-UCLA Medical Center
INTRODUCTION: Although initially developed to gauge risky substance use in adolescents, the CRAFFT questionnaire captures consequences of substance use that are widely applicable in adult populations: use in “cars”, to “relax”, while “alone”, “forgetting”, “family/friends” affected, and “trouble” due to use. Traditional screening methods for substance use measure quantity of use rather than consequences. In this project, we aimed to increase providers’ confidence using CRAFFT in the continuity clinic setting. Specifically, we proposed that using CRAFFT to gauge consequences of substance use would lead to increased rates of SUD diagnosis and treatment.
METHODS: In Oct - Nov 2025, residents and attendings were asked to complete a pre-intervention survey in which they estimated the proportion (0-100%) of patients screened, diagnosed, and treated for tobacco use, alcohol use, and other drug use in their continuity clinics. They also rated confidence (0-100) with screening, diagnosis, and treatment in the same three domains. In late November we held a 45-minute educational intervention about use of CRAFFT in the continuity clinic. Providers were asked to implement the CRAFFT screening from Dec 2025 – Feb 2026; diagnosis and treatment of SUD in screened patients were tracked over this time frame. Residents and attendings then completed a post-intervention survey allowing for comparison of diagnosis/confidence ratings before and after the intervention.
RESULTS: Following the intervention period, providers rated higher levels of engagement and confidence with discussing, diagnosing, and treating SUD on 11 out of 12 domains. The analysis of patients’ CRAFFT responses demonstrated that patients who reported having “family/friends” affected by use were significantly more likely to use substances to “relax” (r=0.73, <0.001), patients with a diagnosis of meth use were significantly more likely to have a diagnosis of tobacco use (r=0.68, <0.001), patients with opioid use disorder were significantly less likely to have a diagnosis of AUD (r=-0.43, <0.001), and patients who accepted a prescription of MAT for AUD were significantly more likely to report using alcohol to relax or had gotten in trouble due to use (r=0.72, <0.001).
CONCLUSIONS: This intervention provided education for family medicine residents and attendings regarding use of the CRAFFT questionnaire to help identify patients with known consequences of substance use disorders. Increased provider engagement and confidence with SUD screening during this project highlights the need to focus more on consequences of substance use rather than quantity, as this method allows providers to rapidly identify patients who would benefit from pharmacologic treatment and community resources.
Launching Park Rx Los Angeles County: Developing and Integrating Key Contractual Components into Formal Agreements of a Community-Clinical Physical Activity Referral Model to Serve the County’s Safety Net Population
AUTHORS: Tony Kuo, MD, MSHS (1)(2)(3), Eloisa Gonzalez, MD, MPH (3), Lisa Arangua, MPP (3), Rebecca Reeves, PT, MPT (3), Samantha Bonilla-Rivas, MPH (3)
AFFILIATIONS: (1) UCLA Fielding School of Public Health; (2) Department of Family Medicine, UCLA David Geffen School of Medicine; (3) Los Angeles County Department of Public Health
INTRODUCTION: Physical inactivity remains a leading contributor to chronic disease, and health systems seek scalable approaches to connect patients to accessible community-based physical activity. Park Rx Los Angeles County (Park Rx LAC) was developed as a park prescription model for the safety-net population supported through formal agreements among large entities, including the County of Los Angeles, the California State University system and community colleges, and city/County parks. Each partner operates within defined administrative structures that limit flexibility, making agreement development complex yet central to implementation success.
METHODS: We conducted an implementation analysis for 2024–2025, focused on the development of formal agreements supporting Park Rx LAC. Data sources included executed and unexecuted agreements, negotiation records, and structured reflections (e.g., PSDA cycles) from stakeholders across public health, higher education, and the parks sector. The Los Angeles County Department of Public Health (DPH) led partner engagement and agreement development. Barriers and facilitators encountered during drafting, legal review, and negotiations were systematically documented and coded using thematic analysis and synthesized into key lessons to inform implementation.
RESULTS: Agreement development revealed consistent challenges across large public sector systems. Initial efforts to establish three-party agreements among healthcare, education, and city parks were overly complex and not executed. Transitioning to multiple two-party agreements improved feasibility, including leveraging existing County intra-agency agreements to facilitate program implementation. Although DPH was initially a project coordinator and evaluator, education and parks partners eventually requested DPH be a formal party, enabling alignment, quality control, and influence on agreement language. Liability coverage for faculty, students, and participants required explicit definition. And foundational contracts with education partners as champions facilitated agreement execution.
CONCLUSIONS: Developing formal agreements across large public sector entities is a central and complex determinant of Park Rx LAC implementation. Structuring partnerships as two-party agreements, formally engaging convening agencies, explicitly addressing liability, and leveraging education-sector champions represent key facilitators. Identifying and leveraging existing agreements were critical to program launch. These lessons offer practical guidance for building sustainable, cross-sector partnerships that support scalable community-clinical physical activity programming for the safety net population.
Whether the Level of Procalcitonin Correlates with Specific Bacterial Diagnoses in the Setting of Septic Patients. A Retrospective Study
AUTHORS: Cecilia Goyette, DO and Amber Williams, DO
AFFILIATIONS: Dignity Health - Northridge Medical Center
INTRODUCTION: Procalcitonin has been used to help guide antibiotic use and support antibiotic stewardship. However, studies regarding its efficacy in this setting have yielded mixed results. Prior studies have not investigated whether a relationship exists between the quantitative value of procalcitonin and specific sepsis diagnoses. If there is a relationship between the level of procalcitonin and a particular bacterial infection, this could prove a useful tool in diagnosing the source of the sepsis. This project aims to identify if there is any relationship between the quantitative value of procalcitonin and the source of infection in septic patients.
METHODS: We completed a retrospective data research study looking at adults hospitalized at Northridge Hospital Medical Center between January to June 2024 who were diagnosed with septicemia or severe sepsis (as labeled with following MS-DRG codes 870, 871, 872) and had procalcitonin levels drawn on the day of admission. Patient inclusion involved matching a Cerner lab report of all procalcitonin labs drawn with a sepsis report containing ICD-10 discharge codes for septic patients during the same period. Only patients common to both lists were included. The final data set included 293 patients who met the inclusion criteria. The cases were then retrospectively categorized into eight major diagnostic groups based on the discharge diagnosis (see results for details on eight groups).
RESULTS: Of the 293 patients that were included for analysis, cases were broken down into the following categories of infection based on discharge diagnosis: 142 cases of pneumonia, 55 cases of GU/UTI, 7 cases of intraabdominal, 17 cases of skin/soft tissue, 14 cases of viral pneumonia, 29 cases of unspecified, 28 cases of multiple etiologies and 1 other. The data was then analyzed using Kruskal-Wallis H Test to compare the eight different categories. H-Statistic was 6.113 with a p-value of 0.41070 indicating that results were not statistically significant, therefore, no clinical significance was found between the values of procalcitonin in the different categories.
CONCLUSIONS: Based on the data and statistical analysis, no apparent differences can be concluded regarding the different groups. The presence of multiple groups with small sample size (less than 20) represents a limitation of the study, especially in comparison to the much larger pneumonia group. The data also showed a wide range of values between the minimum and maximum procalcitonin across multiple groups. Therefore, no relationship between levels of procalcitonin and any specific diagnosis category can be concluded based on this study.
Food Insecurity in Formerly Unhoused Veterans Living in Permanent Supportive Housing: A Quality Improvement Study
AUTHORS: Mia Hoffmann, MSN, FNP-C (1); Irina Haack, MSN, PMHNP-BC (1); Michele Twitchell, MSN, PMHNP-BC (1); Peter Capone-Newton, MD, PhD (1,2); Kristen Kopelson, DNP, ACNP-BC, FNP-BC, FAANP (1); Cleo Penamon, PharmD (1); Jane Luetchens, MSN, PMHNP-BC, PMHCNS-BC (1); Lillian Gelberg, MD, MSPH, FAAFP (1,3)
AFFILIATIONS: (1) UCLA/VA Center of Excellence for Training and Research in Veteran Resilience and Recovery; (2) UCLA David Geffen School of Medicine, Department of Preventative Medicine; (3) UCLA David Geffen School of Medicine and Fielding School of Public Health, Department of Family Medicine
INTRODUCTION: Despite access to on-site food resources, formerly unhoused Veterans living in permanent supportive housing (PSH) continue to screen positive for food insecurity. Standardized screening tools are widely used, yet variability in screening practices and inconsistent follow-up across care settings may limit their effectiveness in identifying and addressing unmet needs. The drivers of this persistent pattern remain unclear. We aimed to define the current state of food insecurity screening and resource utilization among Veterans in permanent supportive housing receiving care in a Homeless Patient Aligned Care Team (HPACT).
METHODS: This quality improvement project followed SQUIRE 2.0 guidelines and used a 9 Box A3 framework to guide current state assessment. We conducted chart reviews of Veterans to evaluate food insecurity screening, documentation of screening outcomes, and follow-up after positive screens among Veterans in PSH enrolled in HPACT. Structured telephone interviews with Veterans using a structured guide clarified responses to the Hunger Vital Sign food insecurity screener. Additional data came from interdisciplinary staff interviews and site visits to on-site food resources. Findings were organized to identify gaps in screening practices, documentation, follow-up and resource utilization.
RESULTS: The current state revealed substantial variability in food insecurity screening practices and follow-up across care settings. Over 25% of Veterans who screened positive had no documented or standardized follow-up. Among those with documented follow-up, dispositions varied widely, including Veterans already receiving assistance, declined referrals, and unclear outcomes. Notably, many Veterans already receiving assistance continued to screen positive, suggesting barriers to resource utilization rather than access. Identified barriers included cognitive impairment, transportation limitations, physical disability, and inconsistent communication of available resources.
CONCLUSIONS: Despite an availability of resources, food insecurity among Veterans living in PSH persists. This highlights gaps in screening, documentation, follow-up, and resource utilization. Inconsistent workflows and unclear follow-up processes contribute to missed opportunities to address food insecurity. Defining the current state identified system-level barriers that will inform targeted quality improvement interventions to standardize workflows, improve follow-up, and enhance resource linkage. Identifying individual barriers may advance development of targeted interventions for this population.
Magic and Machines: A Gamified, AI Enhanced Workshop for Resident QI and Research
AUTHORS: LeMar Hamilton, MD; Klevin Roger Reyes, MD; Lauren Joseph, MD; Alexandra Rabotin, MD, MPH
AFFILIATIONS: Mission Community Hospital, Department of Family Medicine
INTRODUCTION: Artificial intelligence (AI) has emerging potential to support medical education through scalable content generation and learner-centered tools (1). Concurrently, gamification and innovative educational strategies may improve participant engagement and educational outcomes (2). We combined these approaches to design a practical, low-resource workshop aimed at improving residents’ confidence in generating quality improvement and research ideas. We then evaluated whether this workshop improved residents’ perceived ability to generate QI/research ideas and identify learner priorities for future scholarly support.
METHODS: We designed a gamified, Harry Potter–themed quality improvement (QI) and research workshop for family medicine and transitional year residents. The workshop centered around 3 structured deliverables: (1) idea generation, (2) feasibility filtering, and (3) development of a brief project plan with a 60-second pitch. It was inspired by innovation frameworks and techniques (e.g., hackathons) and guided by the five feasibility questions proposed by Horstman et al. (3). ChatGPT (version 5.2) and Gemini (version 3) were used in the workshop design and development of workshop materials, with all content reviewed by the authors. Following the workshop, participants completed an anonymous survey assessing perceived usefulness (4-point Likert scale) and priorities for future scholarly support.
RESULTS: The workshop was conducted on November 7, 2025 during resident didactics and lasted two hours. Eighteen residents completed the post-workshop survey (75% response rate). Twelve of 18 participants (67%) reported the workshop was very helpful, and 6 of 18 (33%) reported it was somewhat helpful in formulating QI and research ideas.
When asked about future priority areas, residents most frequently selected transforming ideas into complete projects (64.7%, n = 11) and use of artificial intelligence tools in research (58.8%, n = 10), followed by data collection and analysis fundamentals (29.4%, n = 5), navigating institutional review board processes (23.5%, n = 4), and preparing posters or presentations (23.5%, n = 4).
CONCLUSIONS: A gamified, AI-supported QI and research workshop was feasible and perceived as helpful for generating scholarly ideas. Participants identified project implementation and artificial intelligence tools as priorities for future training. This low-resource approach may inform residency curricula that support scholarly engagement.
Improving Musculoskeletal Injection Competency in Family Medicine Residents through a Structured Educational Intervention: An Observational Study at Kaiser LAMC
AUTHORS: Debbie Meskin, DO; Nick Hu MD ; Cody Webb MD; Pedro Castellanos MD; Thomas Bird MD; John Su MD
AFFILIATIONS: Kaiser Permanente Los Angeles Family Medicine
INTRODUCTION: Musculoskeletal (MSK) complaints are among the most common conditions managed in primary care, yet many family medicine residents report low confidence in performing joint injections. We aim to evaluate the impact of a four-part lecture and hands-on workshop series (June 2025-February 2026) on residents’ confidence, knowledge, and frequency of performing landmark-guided MSK injections, specifically anatomic guided knee, shoulder, and elbow injections. We hypothesize that the introduction of the structured educational series will improve resident confidence, knowledge and frequency of performing landmark-guided MSK injections.
METHODS: This medical education research project evaluates the effectiveness of a lecture series on knowledge, frequency, and confidence of common landmark-guided MSK injections. Kaiser LAMC Family Medicine residents in the classes of 2025-2028 (36 participants) were evaluated. Data was collected through google forms via a voluntary survey that evaluated frequency and confidence performing anatomic guided knee, shoulder, and elbow injections, as well as 10 knowledge-based questions. Outcome variables included score on knowledge assessment and rate of change of frequency/confidence of injections using descriptive statistics and paired T-test. Outcomes were compared to Class of 2025 pre-intervention scores, along with intra-cohort improvements before and after exposure.
RESULTS: Pre and post survey responses have been collected, and data is being actively reviewed at the time of submission of this abstract. We plan to compare knowledge assessment scores from pre and post surveys for individuals as well as per class. Additionally, we will compare confidence and frequency of each landmark-guided injection pre and post survey. We hope to see improvement of knowledge assessment scores, as well as positive rate of change for confidence and frequency of injections, between individual scores, intra-cohort, and compared to Class of 2025 (control group).
CONCLUSIONS: Conclusions are pending data analysis. We anticipate significant improvements in resident confidence, knowledge scores, and frequency of injections. We also expect these findings to support additional longitudinal, hands-on MSK workshops to improve resident knowledge, confidence, and procedural frequency. Observationally, we noted decreased confidence in MSK examinations for these joints. Future lectures should include MSK exam–focused instruction alongside landmark-guided teaching.
Preventing Patient Misidentification Across Care Settings: Analysis of Near-Miss and Low-Harm Events
AUTHORS: Shalom Katas, MD
AFFILIATIONS: Department Of Family Medicine, CDU
INTRODUCTION: Patient misidentification is a preventable source of medical error across care settings. Risk increases when patients share similar names or demographics, particularly under time pressure and workflow interruptions. Near-miss and low-harm events reveal system vulnerabilities that may otherwise go unrecognized. This study examines safety incidents involving misidentification to identify contributing factors and inform improvement strategies.
METHODS: A retrospective review of three safety incidents was conducted across inpatient and outpatient settings. These included: (1) an inpatient event involving two patients with identical last names, in which an incorrect NPO order was placed, resulting in unnecessary fasting; (2) an inpatient near-miss involving patients with similar letter patterns in their names, in which a procedure order was placed on the wrong patient but intercepted prior to intervention; and (3) an outpatient pediatric near-miss involving patients with identical last names, age, and sex, in which incorrect chart selection led to a planned vaccination for the wrong patient, identified and corrected prior to administration. Root cause analysis was performed.
RESULTS: Contributing factors included reliance on name recognition, inconsistent use of two-patient identifiers, similarity in patient demographics, and electronic health record selection errors. Workflow interruptions and time pressure further increased risk. These factors led to incorrect patient selection, resulting in one low-harm event (unnecessary fasting) and two near-miss events intercepted prior to intervention.
CONCLUSIONS: Patient misidentification occurs across care settings and is driven by similar identifiers and workflow strain. Strengthening verification processes, improving electronic health record safeguards, and reducing interruption-related errors may mitigate risk. Analysis of near-miss and low-harm events provides opportunities for system-level improvement and prevention of future harm.
Implementing “Brown Bagging” in a Primary Care Setting to Improve Chronic Condition Medication Management
AUTHORS: Andre Khawam, DO, Judy Ly, DO, Elaine Roh, MD, Jesse Cheung, MD
AFFILIATIONS: Pomona Valley Hospital Medical Center FMRP
INTRODUCTION: The practice of “brown bagging” describes providers requesting patients to bring their medications into their visits. Brown bagging is intended to obtain accurate medication reconciliation. Accurate medication reconciliation represents a vital component to effectively treat patients and ensure patient safety. Providing patients with a physical bag at their office visits and requesting that they place all of their prescribed medications into their bag for follow up visits can serve to ensure accurate medication reconciliation, reduce polypharmacy, and improve medication adherence and chronic condition management.
METHODS: The study aims to evaluate the effectiveness and barriers of the brown bagging approach in improving medication reconciliation among patients with polypharmacy. The design was chosen to observe the impact of this intervention on medication adherence, accuracy, and patient safety. The inclusion criteria for this study will include all individuals taking 5 or more medications, who do not normally (without being asked to or on their own volition) bring their medications in to their doctor visit. Patients presenting to the Pomona Valley Family Health Center who meet the inclusion criteria will be given a bag to use to carry their medications to doctor visits. They will be instructed to bring the bag to their follow up appointment with all medications inside for review at follow up.
RESULTS: Results for this study will be tracked via a physical tracking document placed in each clinic "POD" to be easily accessible to providers in their group workstations. The tracking documents list the following: date of which medication bag was provided, MRN of patients provided with bag, a check box specifying if medication bag was brought into clinic at follow up appointment, and a check box regarding whether the medication reconciliation in the EMR is accurate. To help facilitate better tracking and awareness amongst providers in the clinic, 2 standardized “dot phrases” will be used in each clinic note in the EMR and listed in the assessment and plan of clinic notes for each patient’s provided medication bags.
CONCLUSIONS: Prior to the study, medication reconciliation was not being regularly done utilizing the formal EMR feature, which makes medication reconciliation efforts difficult to track. Currently, the assessed barriers to improved medication reconciliation in the setting of polypharmacy are additional time taken to review medications in brown bags and update the tracking sheet. We hope by brown bagging, our patients' efforts will translate to providers more consistently updating the EMR medication reconciliation.
Use of Proton Pump Inhibitors and Fracture Risk – Subgroup Analysis
AUTHORS: Allison Siu, DO; Irfan Habib, DO; Eunice Kim, DO; Stephanie Chen, MD; Jin Kim Paglingayen, MD; Laura Nader, MD
AFFILIATIONS: Riverside University Health System/UCR
INTRODUCTION: Proton pump inhibitors (PPIs) are medications that irreversibly inhibit acid-secreting channels in the stomach and alleviate pain as seen in gastroesophageal reflux disease. Given their well-tolerated side effect profile, use of PPIs is often extended beyond the recommended 3 months of continuous use. However, they have been correlated with increased incidence of fracture. Prior analysis of the population at Riverside University Health System (RUHS) did not show statistically significant increase in fracture risk with long term use of PPIs. The aim of this study is to perform a subgroup analysis by body mass index (BMI) ranges.
METHODS: Epic EMR was used to perform a cohort retrospective analysis of the RUHS patient population. Our inclusion criteria were patients ages 18-65 years old receiving care at RUHS Community Health Centers and prescribed a PPI. Our exclusion criteria were patients less than 18 years old and greater than 65 years old with a diagnosis of osteopenia. Further, a subgroup analysis was performed to identify if there is an increased risk of fracture in patients using long term PPIs based on different BMI ranges: underweight (BMI < 18.5), normal weight (BMI 18.5-24.9), overweight (BMI 25-29.9), obesity (BMI>=30).
RESULTS: Slicer Dicer was used to compare rates of fracture among underweight, normal weight, overweight, and obesity. Results showed highest rate of fracture among the underweight group with an odds ratio of 5.788 and lowest rate of fracture among the obesity group with an odds ratio of 0.91. There was a statistically significant difference in the odds ratio when comparing the group with BMI 25-29.9 and the group with BMI>=30. The odds ratios of the group with BMI 25-29.9 and BMI >=30 were statistically significant to the groups with BMI <18.5 and BMI 18.5-24.9. There was no statistically significant difference in the odds ratio when comparing the group with BMI <18.5 and the group with BMI 18.5-24.9.
CONCLUSIONS: Per review of literature, there has been evidence showing that being underweight is a risk factor for fracture in men and women. Hip fracture rates were lower in overweight and obese categories compared to normal weight. Our subgroup analysis showed decreased rates of osteoporosis with pathologic fracture in patients with obesity which supports the literature that there are lower rates of fracture in patients with higher BMIs. Thus, when prescribing PPIs in the outpatient setting, a patient’s BMI should be considered when discussing risks and benefits of use.
Two Heads Are Better Than One: A Teamlet Approach to Cognitive Health Screening in an Urban Underserved Family Medicine Teaching Clinic
AUTHORS: Heather Schickedanz, MD; Anthony Kim, MD; Sa Heen Park, MD; Neiki Rokni, MD; Isabell Holguin
AFFILIATIONS: Department of Family Medicine, Harbor-UCLA
INTRODUCTION: Cognitive impairment affects millions of older adults yet often goes undetected in primary care. Approximately 10% of adults ≥65 years have dementia, with a larger proportion affected by mild cognitive impairment, many undiagnosed in routine care.¹ Although cognitive health screening is incorporated into the Medicare Annual Wellness Visit for beneficiaries ≥65 years, real-world uptake remains low at 20–30% annually.²⁻⁴ Implementation barriers include time constraints, inadequate training, and lack of structured workflows.⁵ This study evaluates a nurse-led teamlet approach to increase CHS completion in an urban family medicine teaching clinic.
METHODS: We conducted a retrospective chart review of randomly selected visits for patients aged 65 years from August 2025 to January 2026 at an urban teaching clinic. Outcomes included completion of nurse-led CHS and physician attestation. Interventions included staff education, workflow redesign, incentives, and electronic and paper-based reminders. Analyses examined variation by age, primary language, and provider type using descriptive statistics.
RESULTS: Among 349 visits, 316 (90.5%) included nurse-led CHS, demonstrating high screening uptake. Physician attestation occurred in 156 visits (49.4%), identifying a significant gap in provider follow-through. The population was predominantly Spanish-speaking (51.0%). Preliminary analyses show variation in attestation rates by provider type and over time. No major adverse workflow disruptions were observed.
CONCLUSIONS: A nurse-led teamlet model improved cognitive health screening rates in an urban teaching clinic. However, gaps in physician attestation persist, limiting full implementation. Targeted workflow improvements may enhance provider engagement and promote equitable dementia care. This approach offers a scalable model for improving screening delivery in diverse primary care settings.
Does The Usage of Home Diuretics Affect Length of Stay for Patients with Acute Kidney Injury
AUTHORS: Tristan Copeland; Daniel Tellez; Lawrence To; Darian Mangu; Uziel Sauceda
AFFILIATIONS: RUHS Medical Center; RUHS/UCR Family Medicine Program
INTRODUCTION: Etiologies of AKI include those that are expected to improve with volume, and those that will improve with time and removal of an offending agent. We suspect that in patients admitted with AKI at RUHS medical center there is a significantly longer time to downtrend of the serum creatinine between patients who were on home diuretics versus patients who were not on home diuretics. The following study aims to evaluate for a significant difference in time to downtrend of serum creatinine at RUHS Medical Center between individuals both receiving and not receiving home diuretics when controlling for chronic comorbidities.
METHODS: Mann-Whitney U test will be used to compare continuous variables while Pearson’s chi-square (Bonferroni's correction) will be used to compare categorical variables; Fisher’s exact test for infrequent occurrences. A p value of ≤0.05 will be considered significant. The statistical software SPSS will be used as the primary data analysis tool. Instances of missing data <5% will be deemed negligible.
RESULTS: Results pending.
CONCLUSIONS: Conclusions pending further results.
Catalina Room - Case Reports
Bent Out of Shape: Pseudoarthrosis in an Unsheltered Patient. Challenges and Management in Street Medicine
AUTHORS: Luis Chaviedo Gutierrez, MD (1), Kyung Hwan Kim MD (1), Rachel Battersbersby MSIII (2), Harnek Singh MD (1)
AFFILIATIONS: (1) Rio Bravo Family Medicine Residency Program; (2) Western University of Health Sciences
INTRODUCTION: Pseudoarthrosis represents a failure of bone healing resulting in a false joint, often associated with inadequate stabilization, poor vascular supply, or patient-related factors such as malnutrition and limited access to care. While commonly discussed in orthopedic literature, pseudoarthrosis in underserved populations, particularly within street medicine, remains underreported. Barriers to follow-up and continuity of care significantly increase the risk of delayed complications and poor outcomes.
METHODS: We present the case of an adult patient experiencing homelessness who was encountered through a street medicine program with persistent lower extremity pain and deformity following a prior untreated fracture. The patient reported a history of trauma several months prior but did not seek or receive formal medical care at that time. On examination, there was visible deformity of the affected limb with abnormal mobility at the site of injury, consistent with a nonunion. The patient endorsed chronic pain, impaired ambulation, and progressive functional limitation. Imaging confirmed pseudoarthrosis with malalignment of the affected bone. Given the patient’s social circumstances, including housing instability and limited access to healthcare, management posed significant challenges. The patient was connected with multidisciplinary services, including orthopedic surgery, social work, and care coordination, to facilitate definitive management and follow-up.
DISCUSSION: This case highlights pseudoarthrosis as a preventable complication of untreated fractures, particularly in vulnerable populations. Patients experiencing homelessness face barriers to timely diagnosis, treatment adherence, and follow-up care. Street medicine programs play a key role in identifying these conditions, bridging care gaps, and coordinating multidisciplinary management. Early recognition and engagement are essential to improving outcomes. This case underscores the need to integrate social determinants of health into clinical decision-making and expand outreach to underserved populations. Pseudoarthrosis in this setting reflects both clinical and systemic gaps in access to care, requiring targeted outreach and coordinated interventions.
Don't Forget the Worms: Trichuris trichiura Causing Life-Threatening Anemia in a Non-Endemic Area
AUTHORS: Andrea Collingwood, DO; Nancy Rodriguez, MD, MPH, MBA, MHA; Ferina Farahnik, DO; Matthew Yu, DO, MPH, DipABLM, FAAFP
AFFILIATIONS: Department of Family Medicine at Charles R. Drew University of Medicine and Science; LAC-DHS Martin Luther King Jr. Outpatient Center
INTRODUCTION: Trichuris trichiura remains an under-recognized cause of severe iron deficiency anemia (IDA) outside endemic regions. We present a 70-year-old Guatemalan woman with refractory IDA (presenting hemoglobin 3.8 g/dL) whose etiology was unidentified for over one year in part due to loss of access to insurance. Colonoscopy revealed massive whipworm infestation with co-infection by hookworm and Blastocystis hominis. This case underscores the importance of epidemiologic and travel history, including potential parasitic exposures, in the workup of unexplained anemia.
METHODS: A 70-year-old Guatemalan woman with chronic IDA, right lower extremity amputation, and neurocysticercosis presented with presyncope and confusion. She had relocated from Guatemala to the United States in 2024, with no subsequent travel. She had a similar episode one year ago and received a blood transfusion but did not complete workup due to loss of insurance. She denied overt bleeding or weight loss. Laboratory evaluation revealed a critically low hemoglobin, iron studies consistent with IDA, and peripheral eosinophilia. She received 3 units of pRBC. Esophagogastroduodenoscopy showed mild gastritis and grade A esophagitis; H. pylori was negative. Colonoscopy revealed numerous motile worm-like organisms from transverse colon to cecum. Further history revealed prior exposure to raw pork and unpasteurized pork milk during childhood. The patient was treated with albendazole and ivermectin. Stool ova and parasite studies confirmed numerous Trichuris trichiura, few hookworms, and many Blastocystis hominis. She was discharged with the remaining albendazole course and outpatient follow-up.
DISCUSSION: This case highlights the diagnostic challenge of parasitic infections outside endemic areas. Trichuris trichiura infects over 800 million people globally, with highest prevalence in Central America, sub-Saharan Africa, and Asia. Chronic infections acquired in early life can persist for years after relocation from endemic areas. Heavy worm burden causes occult colonic blood loss and impaired iron absorption, producing refractory IDA and in severe cases Trichuris Dysentery Syndrome. Co-infection with hookworm and Blastocystis hominis may further contribute to malabsorption. Refractory IDA with eosinophilia should prompt clinical suspicion for helminthiasis. Detailed epidemiologic history, including early environmental exposures, is essential to guide appropriate workup and timely treatment.
Reversible High-Grade Heart Block and Resolution of Chronic Symptoms in Stage 2–3 Lyme Disease
AUTHORS: Yuntao Dai, MD PhD (1), Maggie Torsney-Weir, MD (1), Akash Goyal, MD (2), Konstantinos Boudoulas, MD (2), Richard Gumina, MD PhD (2)
AFFILIATIONS: (1) Department of Family Medicine at Mission Community Hospital; (2) Division of Cardiovascular Medicine at The Ohio State University Wexner Medical Center
INTRODUCTION: Lyme disease, caused by Borrelia burgdorferi and transmitted by Ixodes ticks, is the most prevalent tick-borne disease in the United States. We report a unique case with a patient presenting with the full triad of arthritis-like symptoms, cardiac conduction block, and alpha-gal syndrome. He achieved complete clinical and functional recovery following antibiotic therapy. This case highlights the importance of maintaining a broad differential diagnosis and timely treatment in primary care settings.
METHODS: A 48-year-old male presented to the emergency department with three episodes of asystole. His past medical history was notable for chronic arthritis refractory to acetaminophen and a severe beef allergy unresponsive to loratadine. Social history revealed a decade-long occupation as a rural truck driver with frequent tick exposures. Electrocardiography demonstrated third-degree atrioventricular (AV) block. Electrophysiologic studies confirmed infra-Hisian conduction failure. Lyme serology, including ELISA and confirmatory Western blot, returned positive. Given the high suspicion for Lyme carditis, intravenous ceftriaxone was initiated empirically. A temporary transvenous pacemaker was placed for prophylaxis against further AV block progression. Over a two-week course of ceftriaxone, the patient’s PR interval progressively normalized to <200ms. Repeated electrophysiology study confirmed recovery of AV nodal conduction. He was stably discharged with two-week course of doxycycline.
DISCUSSION: Timely recognition and antibiotic therapy reversed advanced cardiac involvement in this patient, with concurrent resolution of chronic arthritis and beef allergy symptoms, supporting a role for Borrelia-associated immune dysregulation. This finding aligns with prior reports linking Lyme disease to alpha-gal syndrome, a delayed IgE-mediated food allergy to galactose-α-1,3-galactose following tick exposure. To our knowledge, no prior cases have demonstrated remission of alpha-gal syndrome after treatment of B. burgdorferi. This represents the first reported case in which both cardiac conduction block and alpha-gal–related symptoms resolved following antibiotic therapy for Lyme disease.
Beyond Mycoplasma: The Expanding Spectrum of Reactive Infectious Mucocutaneous Eruption (RIME)
AUTHORS: Thomas Bird, MBBS, Nina Fukuma, MD, Patricio Ruano, MD, Justin So, MD, Tara Thacker, MD
AFFILIATIONS: Department of Family Medicine at Kaiser Permanente Los Angeles
INTRODUCTION: Reactive infective mucocutaneous eruption (RIME) is characterized by mucositis involving the oral, ocular, and urogenital mucosa in the setting of an infectious trigger, most commonly Mycoplasma pneumoniae. While most cases occur in the pediatric population, RIME also affects young adults and poses diagnostic challenges due to overlap with Stevens-Johnson syndrome, Behçet disease, and other causes of mucositis. We present the case of a patient who developed severe mucositis in the setting of M. pneumoniae infection, diagnosed as RIME and successfully treated with azithromycin and etanercept.
METHODS: 27 year old female, with history of HSV-1, presented to the ED with fevers, cough, nasal congestion, and sore throat in the setting of recent travel to Indio, CA. Following empiric treatment with amoxicillin and azithromycin, patient presented to the ED on day 12 of symptoms, now with severe bilateral blepharoconjunctivitis with subconjunctival hemorrhage as well as conjunctival, oral, and genital mucositis. Work up was notable for positive Coccidiomycoses IgM, but negative IgG, suggesting a false positive, as well as negative HIV, syphilis, HSV, VZV, murine typhus IgG, and RPP. Patient’s autoimmune work up, including ANA, ANCA, dsDNA, HLAB51, and pathergy test, returned negative, making Behchet’s syndrome unlikely. Infectious work up was notable for positive Mycoplasma IgM (2.32; normal <0.76), suggestive of a highly significant amount of M. pneumoniae antibody. The patient was evaluated by dermatology, ophthalmology, and rheumatology, and found to have RIME. Following treatment with Azithromycin and Etanercept, patient had significant improvement to symptoms.
DISCUSSION: RIME is uncommon, seen in 11-13% of patients hospitalized for M. pneumoniae, most often in children (1,2). Given the broad differential for viral exanthems, recognizing RIME is important for accurate diagnosis and treatment. For example, RIME may be mistaken for SJS/TEN or Behcet’s, and the viral prodrome can resemble Hand-Foot-Mouth (3). Studies demonstrate how serology for M. pneumoniae, as used in our case, may offer greater clinical utility than PCR by capturing current and recent infections (4). Additionally, pediatric case reports show how etanercept, as used in our patient, may reduce pain, length of stay, and expedite diet advancement (5). The use of etanercept in our adult patient warrants further investigation in larger cohorts to establish its efficacy in the adult population.
Occipital Horn Arachnoid Cyst in a Newborn
AUTHORS: Jacquelyn Garcia MD (1,2), Rachel Battersby MS III (3), Rasha Alnajjar MS III (3), Brian Shafter MS III (3), Thiagarajan Nandhagopal MD (1)
AFFILIATIONS: Kern Medical (1), Rio Bravo Family Medicine Residency Program (2), Western University of Health Sciences (3)
INTRODUCTION: Arachnoid cysts are benign, cerebrospinal fluid–filled sacs that account for about 1% of intracranial lesions in children. Most arachnoid cysts occur in the anterior or middle cranial fossae and the retrocerebellar cistern.¹ In contrast, intraventricular arachnoid cysts are exceedingly rare, with only a few cases reported.² These may originate from the arachnoid layer within the choroidal fissure. Here, we present a rare case of a newborn with an arachnoid cyst measuring 4.3 cm × 2.1 cm located in the left occipital horn of the lateral ventricle.
METHODS: A male infant was born at 38w+1d gestation via NSVD after an uncomplicated pregnancy. Prenatal ultrasound performed by MFM revealed left lateral ventricular dilation, measuring 1.7 cm, and growing to 2.2 cm 4 weeks later. An ultrasound encephalogram performed on day 2 of life demonstrated moderate to marked dilation of the left occipital horn. Pediatric neurosurgery at Valley Children’s Hospital recommended further imaging. MRI revealed a dilated left occipital horn containing a well-circumscribed, CSF-intensity cystic lesion measuring 4.3 × 2.1 cm, consistent with an arachnoid cyst.
DISCUSSION: This case is noteworthy due to the unusual location of the cyst within the left occipital horn of the lateral ventricle in a newborn. Few cases have been reported and most are diagnosed later in infancy/childhood. Recognition of this entity is important to avoid misdiagnosis and unnecessary intervention. In our patient, the lesion was detected prenatally as progressive unilateral ventricular dilation and later confirmed postnatally by MRI as an arachnoid cyst. Current management of asymptomatic arachnoid cysts tends to be conservative, emphasizing observation and serial neuroimaging unless there is evidence of mass effect, hydrocephalus, or neurological compromise. Given the large size and rare location in this neonate, close follow-up and workup with a pediatric neurosurgeon is critical.
A Fulminant Acneiform Presentation of Systemic Neutrophilic Inflammation in Mixed Connective Tissue Disease
AUTHORS: Belonwu Okafor, MD; Parastou Farhadian, MD
AFFILIATIONS: Mission Community Hospital, Department of Family Medicine
INTRODUCTION: Severe acneiform eruptions with systemic inflammation are uncommon and can mimic infection, delaying appropriate treatment. Distinguishing between acne fulminans, neutrophilic dermatoses, and infectious etiologies is critical, particularly in patients with autoimmune disease receiving immunomodulatory therapy. We present a case of a fulminant acneiform eruption in a patient with long-standing connective tissue disease, highlighting diagnostic challenges and the importance of early recognition of neutrophilic inflammatory processes.
METHODS: A 36-year-old female with a 15-year history of connective tissue disease with overlap features (inflammatory myositis, lupus-spectrum disease, and Raynaud’s phenomenon) who presented with a 2-week history of rapidly progressive, painful acneiform lesions involving the face, neck, trunk, and palms, associated with impetiginous lesion, fever and constitutional symptoms. Patient had been on upadacitinib prior to onset. Laboratory evaluation showed ESR 120 mm/hr and CRP 17.5 mg/dL with normal WBC. Despite doxycycline and empiric antibiotics (Vancomycin and later Clindamycin), symptoms persisted. Patient received intravenous methylprednisolone with rapid improvement in pain and lesion severity and was discharged on a prednisone taper with outpatient follow-up.
DISCUSSION: The acute onset, ulcerative acneiform morphology, acral involvement, markedly elevated inflammatory markers, and rapid corticosteroid response favored a neutrophilic inflammatory process within the spectrum of acne fulminans and Sweet syndrome rather than infection or uncomplicated acne. Despite long-standing autoimmune disease, the absence of concurrent organ-specific flare and atypical morphology argue against a primary autoimmune etiology. Upadacitinib may have contributed via immune dysregulation. Early recognition of neutrophilic dermatoses is essential to avoid misdiagnosis, unnecessary antibiotics, and inappropriate acne-directed therapy.
Joshua Tree Room - Abstracts
A Self-Paced, Web-Based Knee MRI Interpretation Course Improves Trainee Confidence: A Pilot Study
AUTHORS: Kimberly Burbank, MD; Jeremy Swisher, MD
AFFILIATIONS: Division of Sports Medicine, Department of Family Medicine, David Geffen School of Medicine at UCLA
INTRODUCTION: Knee MRI interpretation is a core competency for sports medicine physicians, yet most training programs lack structured imaging curriculum. Trainees typically develop this skill informally through clinical exposure, resulting in knowledge gaps and low self-reported confidence. Trainees may lack the systematic framework needed to feel confident interpreting MRI independently. This is especially important in sports medicine fellows and residents interested in pursuing sports medicine fellowship. We developed a web-based knee MRI interpretation course to address this confidence gap among UCLA sports medicine fellows and family medicine residents.
METHODS: We developed a competency-based curriculum delivered via a custom web application. The course includes 9 teaching modules covering MRI basics, anatomy, a standardized 7-step search pattern, and pathology across bone, cartilage, menisci, ligaments, the extensor mechanism, and high-yield findings. Learners completed up to 13 graded interactive cases. Five UCLA trainees (1 sports medicine fellow, 4 family medicine residents) completed both the full course and pre- and post-course assessments during the 2025-2026 academic year, including a 13-item knowledge quiz and a 7-domain confidence survey (1-5 Likert scale). Paired t-tests compared pre- and post-course outcomes, and Cohen's d was calculated for effect size.
RESULTS: Among the 5 course completers, pre-quiz scores were high at baseline (mean 87.8%, SD 3.8%), while pre-confidence was low (mean 1.84/5, SD 0.49). Knowledge scores showed a non-significant increase from 87.8% to 89.2% (mean change +1.4pp, p=0.62, Cohen's d=0.24). Self-reported confidence improved significantly from 1.84 to 3.14 (mean change +1.30, p=0.001, Cohen's d=3.83), a 71% relative increase. All 5 completers demonstrated confidence gains of at least 0.9 points. All 7 confidence domains improved, with the largest gains in structured reporting (+1.80), bone marrow patterns (+1.60), and corners/collaterals (+1.60). Mean module quiz performance was 89.8%.
CONCLUSIONS: This pilot demonstrates that a self-paced, web-based knee MRI course produces large, statistically significant improvements in trainee confidence with MRI interpretation. Despite high baseline knowledge (88%), trainees reported low confidence (1.8/5), revealing a knowledge-confidence gap that a structured curriculum can help address. The course produced a significant confidence gain (p=0.001, d=3.83)
Practice Makes Progress: Assessment of Residency Confidence After Ultrasound Curriculum in an Academic Family Medicine Program
AUTHORS: Sessen Dudek MD & Phillip Brown MD
AFFILIATIONS: UCLA Department of Family Medicine
INTRODUCTION: Point-of-care ultrasound (POCUS) is an increasingly valuable tool in clinical practice, providing real-time diagnostic and procedural support. Despite growing interest, implementation of standardized curricula in residency training remains inconsistent. This study evaluates the implementation of a structured ultrasound curriculum to improve resident knowledge and confidence, identify barriers to learning, and inform ongoing development of an effective and sustainable POCUS curriculum.
METHODS: UCLA Family Medicine Residents participated in a newly established 2-week POCUS curriculum comprised of instructional videos, and hands-on scanning sessions.
A pre–post survey study was conducted using Likert-scale items to assess change in confidence pre and post rotation. The survey assessed prior ultrasound experience, barriers to using ultrasound, technical skills (adjusting depth, probe selection), clinical competencies (FAST, AA, Cardiac, MSK etc.), and rotation satisfaction. It also gauged interest in implementation of ultrasound in future practice. This study serves as a quality improvement project to aid the development of a sound and replicable residency ultrasound curriculum.
RESULTS: Paired t-tests showed significant increase in self-reported confidence for gain/depth adjustment (+1.2, p = 0.037), probe selection (+1.0, p = 0.015), paracentesis fluid localization (+0.8, p = 0.037), vascular identification using doppler (+1.3, p = 0.013), and ultrasound-guided knee injection (+0.6, p = 0.005). These were associated with medium to large effect sizes (Cohen’s d = 0.77–1.16).
FAST/eFAST (+0.4, p = 0.104), pericardial effusion diagnosis (+0.4, p = 0.168), basic cardiac view (+0.5, p = 0.052), and abdominal aorta assessment (+0.9, p = 0.054), demonstrated a moderate effect size (d = 0.47–0.71), but without statistical significance.
CONCLUSIONS: A structured 2- week POCUS curriculum demonstrated statistically significant improvements in gain/depth adjustment, probe selection, doppler use, paracentesis localization, and ultrasound-guided knee injections. Other domains showed positive trends without significance. Despite a small sample, this pilot study suggests that a short POCUS curriculum can increase learner confidence. Expanding access to personal probes and integration across other rotations may further enhance the curriculum. Future studies should reassess confidence and utilization at 3 months to evaluate longitudinal impact.
Helping Patients Suffering from Obesity with an Individualized Approach to Lifestyle-Modifications in a FQHC Primary Care Setting
AUTHORS: Lovedip Kooner, MD; Yvette Singh, MD; Stephanie Garcia, MD; Michael Ozoemena, MD; Leopoldo Jose Hartmann, MD; Ejodakeme Okojie, MD; Ranbir Sandhu, MD; Zheng Song, MD; Hector Arreaza, MD; Harnek Singh, MD
AFFILIATIONS: Rio Bravo Family Medicine Program
INTRODUCTION: Obesity contributes to 335,000–500,000 deaths annually in the United States. Although medications are effective, cost and discontinuation limit durability; without sustained lifestyle modifications, weight regain is nearly universal, and 40–50% of patients abandon structured programs within 2 months. Psychological, social, logistical, and healthcare system barriers—compounded by brief primary care visits—undermine change. We hypothesize that a single page hand out utilizing S.M.A.R.T. goals implemented in primary care can transform adherence to lifestyle modifications.
METHODS: Adults 18 years and older with BMI greater than 30 receiving care at a federally qualified health center were invited to enroll during weight management visits in a prospective pre post study. Fifty patients participated. The intervention included a CBT based SMART goal handout used during visits with physician guidance. Surveys in English and Spanish using numeric scales and categorical measures were completed at baseline and 3 months assessing physical activity, unhealthy, meals, fatigue, confidence, and perceived support. Outcomes were analyzed using paired t testing and Wilcoxon signed rank testing for ordinal variables with significance set at p less than 0.05.
RESULTS: Fifty patients completed the study. Confidence increased from 6.86 to 8.80 mean change 1.94 plus minus 1.67 t 50 equals 8.22 p less than 0.001 and perceived support increased from 7.14 to 9.36 mean change 2.22 plus minus 2.36 t 50 equals 6.74 p less than 0.001. Fatigue decreased from 5.64 to 4.20 mean change minus 1.44 plus minus 1.65 t 50 equals minus 6.16 p less than 0.001. Unhealthy meals decreased from 4.46 to 3.10 mean change minus 1.36 plus minus 1.72 t 50 equals minus 5.59 p less than 0.001. Exercise increased with 56 percent improving at least one category p less than 0.001. No adverse events were reported.
CONCLUSIONS: A SMART goal tool-based handout in primary care significantly improved adherence to lifestyle modifications, with increased confidence and perceived support, greater exercise participation, and reductions in fatigue and unhealthy eating. These results suggest that structured behavioral strategies can address common psychological and practical barriers within time limited visits. Integrating simple scalable interventions into routine primary care may enhance patient engagement and support more durable lifestyle change.
Use of Cystatin C to Improve Evaluation of Abnormal Creatinine in Competitive Baseball Players: A Quality Improvement Project
AUTHORS: Kyle Lau, MD; Kimberly Burbank, MD; Alexander Soto, MD MPH; and Marissa Vasquez-Machuca, MD MBA
AFFILIATIONS: Division of Sports Medicine at UCLA
INTRODUCTION: Competitive baseball players may present with elevated serum creatinine values that do not reflect true renal disease, yet may trigger disruptive and costly unnecessary actions including additional testing, specialist referrals, and sport participation restrictions. Serum creatinine is proportional to muscle mass and can be influenced by diet. Cystatin C is produced at a constant rate by all nucleated cells, making it less affected by muscle mass, age, or diet. This project aims to implement a clinical pathway incorporating serum Cystatin C as a reflex test for abnormal creatinine to screen renal function of elite baseball players.
METHODS: 221 male minor league baseball players (between the ages 24 to 38 years old) were screened, 113 in 2025 and 108 players in 2026. In 2025, all players received both creatinine and Cystatin C testing. In 2026, all athletes received a screening creatinine test and a reflex Cystatin C test was done only for players with abnormal creatinine results. Cost of Cystatin C testing was obtained from commercial ($150/test, Quest 2025 pricing) and in-house ($60/test) laboratories. Outcomes included proportion of athletes reclassified as having normal kidney function, frequency of additional diagnostic testing or specialty referral, impact on clearance for athletic participation, and cost-effectiveness.
RESULTS: In 2025, 36 of 113 players (31.9%) were flagged for elevated serum creatinine, but all players had normal Cystatin C values. In 2026, 31 of 108 players (28.7%) had elevated serum creatinine, but all players then had normal Cystatin C values. In total, 67 of 221 players (30.3%) were flagged with abnormal creatinine, and 100% of them were reclassified as having normal kidney function after Cystatin C testing (3 specimens were not received by the lab). This led to no additional diagnostic testing or specialist referrals. The transition to a targeted reflex protocol reduced total Cystatin C tests by 72.6%. Based on 82 fewer Cystatin C tests performed, estimated cost savings were approximately $12,300 using commercial laboratory pricing or $4,920 using in-house institutional pricing.
CONCLUSIONS: Following implementation of this project, all baseball players previously flagged for abnormal renal function based on creatinine were reclassified as having normal kidney function using Cystatin C, resulting in fewer unnecessary interventions, reduced specialist referral burden, and accurate sport participation decisions. Using Cystatin C reflex testing for abnormal creatinine results reduced overall cost. This project demonstrates that incorporating Cystatin C to screen elite baseball players’ renal function improves diagnostic accuracy and is cost-effective.
Improving Clinic Cycle Time and Team-Based Efficiency Through Agenda Setting in an Ambulatory Resident Clinic: Perspectives of Nursing Staff
AUTHORS: Nancy Rodriguez, MD, MPH, MBA, MHA; Jackline Muthoka, MD, MBA; Shalom Katas, MD; Adriana Rodriguez, MD; Matthew Yu, DO, MPH, DipABLM, FAAFP; Karamjit Chela, MD, MPH
AFFILIATIONS: Department of Family Medicine at Charles R. Drew University of Medicine and Science, LAC-DHS Martin Luther King Jr. Outpatient Center
INTRODUCTION: Prolonged wait-times and inefficient clinic flow drive patient dissatisfaction and staff burden in outpatient family medicine. Unstructured resident visit agendas are a modifiable contributor to delays. Nursing staff directly experience the effects of visit inefficiency through patient frustration, delayed room turnover, and clinic sessions extending beyond scheduled end times. Despite their frontline operational role, nursing perspectives are rarely included in residency quality improvement efforts. This study evaluates the impact of a structured resident agenda-setting intervention on nursing perceptions of clinic efficiency.
METHODS: This prospective pre/post survey study included all nursing staff (estimated n=8–15). Participants completed a locally developed Likert-scale survey before the intervention (April 2026) and approximately three weeks after implementation (late April–early May 2026). Survey domains included perceived patient wait time from check-in to rooming, resident visit duration and its downstream effects on clinic flow, and on-time clinic completion, including sessions extending >30 minutes past scheduled end. Two open-ended questions assessed perceived causes of delays and suggested workflow improvements. Descriptive statistics will be used for pre/post comparisons. This is one of four companion QI studies evaluating the same intervention alongside faculty, nursing, and objective cycle-time measures.
RESULTS: Data collection is ongoing. Baseline data (Jan–Feb 2022) identified Monday afternoon PGY-2 clinics as highest workload, with staff frequently exceeding scheduled hours (>30 minutes). Tuesday PGY-1 sessions required increased preceptor support (3 preceptors/session) and demonstrated the longest mean cycle times. Staff reported delays driven by prolonged resident visits and inefficient agenda setting. These findings highlight workflow bottlenecks contributing to staff overtime and delayed clinic completion. Post-intervention survey results and comparative analyses will be available at the time of presentation.
CONCLUSIONS: Baseline findings demonstrate structural inefficiencies and uneven workload distribution in resident clinics. Targeting upstream factors such as agenda setting may improve clinic flow and reduce staff burden. Nursing staff offer a critical and often underutilized operational perspective, as they directly experience delays in patient flow, room turnover, and session overruns. Incorporating nursing feedback as a formal outcome measure broadens evaluation beyond administrative cycle-time metrics and supports sustainable, team-based quality improvement in resident continuity clinics.
Before the Crisis: Cultivating Resident Confidence in Outpatient Advance Care Planning
AUTHORS: Jasmine Nevarez, MSPH MD; Menna Sharafeldeen, DO; Heather Schickedanz, MD;
AFFILIATIONS: Department of Family Medicine, Harbor-UCLA
INTRODUCTION: Due to increased patient complexity and lifespan, there is greater need for advance care planning (ACP) discussions between patients and medical care teams to promote goal-concordant care. However, resident physicians may face difficulties initiating conversations in the outpatient setting due to competing clinical priorities and lack of education or familiarity with ACP. Residents often struggle to initiate advance care planning outside of acute inpatient crises or end-of-life scenarios. Educational interventions have been shown to improve resident confidence and increase outpatient ACP discussions.
METHODS: Harbor-UCLA Family Medicine Residents and Faculty participated in a brief didactic on ACP, and completed an anonymous 11-item pre- and post- survey. Eight of the questions evaluated participant attitudes on a numerical scale from 1 to 10. The last three questions were free responses for session feedback and perceptions of barriers to ACP. The pre- and post- surveys mean scores were compared in a t-test analysis with a p-value < 0.05 indicating significant differences. Only participants that completed pre- and post- surveys were included in analysis. A qualitative analysis was performed of free response answers to evaluate common responses and themes.
RESULTS: Of the twenty-one participants, only 7 completed both the pre- and post- surveys. Despite the small sample size, following the educational intervention there was a statistically significant increase in scores indicating increased confidence and knowledge after the session in all topics, including knowledge of various ACP documents, initiating both outpatient and inpatient ACP discussions, and ACP billing. Qualitative analysis revealed that the most common barriers to outpatient ACP were limited clinical time and a perceived lack of patient readiness. Participants expressed appreciation for the training on ACP discussions and guidance on relevant billing codes.
CONCLUSIONS: Advance care planning is a core component of quality, patient-centered primary care. Family Medicine residents frequently engage in ACP discussions with patients in the inpatient setting or during clinically acute times, when it is more challenging to elicit patients’ wishes. By improving resident knowledge and confidence, physicians in training can learn to initiate proactive, goal-concordant care and ACP discussions in continuity clinics. Facilitating these conversations with appropriate tools and billing education ensures continuity of patient-centered care before an acute crisis occurs.
Electronic Hand Hygiene Monitoring and Compliance Among Resident Physicians: A Pre–Post Quality Improvement Study
AUTHORS: Raymond Phan, DO; Amber Williams, DO, FAAFP, FHM
AFFILIATIONS: Dignity Health - Northridge Medical Center
INTRODUCTION: Hand hygiene is a cornerstone of infection prevention and a critical determinant of patient safety, yet compliance among physicians remains inconsistent across healthcare settings. Traditional monitoring methods, including direct observation, are limited by observer bias, resource constraints, and the Hawthorne effect, often overestimating true adherence. Electronic monitoring systems offer continuous, objective measurement of hand hygiene behavior, but their effectiveness among resident physicians remains unclear. This study evaluates whether implementation of electronic monitoring with feedback improves compliance in this population.
METHODS: We conducted a quality improvement–focused observational pre–post study at a single academic medical center. Resident physicians were monitored using an electronic hand hygiene system utilizing wearable badges and dispenser-based sensors. A 4-week baseline phase with passive monitoring and no feedback was followed by a 10-week intervention phase with introduction of aggregate compliance feedback. Weekly hand hygiene compliance data were collected and analyzed in aggregate. The primary outcome was change in compliance between baseline and intervention phases. Comparisons were performed using a two-proportion z-test to assess statistical significance.
RESULTS: A total of 14 weeks of data were analyzed. During the baseline monitoring phase, aggregate hand hygiene compliance among resident physicians was 72.3%. During the intervention phase, compliance decreased to 67.1%, representing an absolute decrease of 5.2%. Statistical analysis demonstrated that this difference was significant (p < 0.001). Weekly compliance trends showed a gradual decline over the study period following introduction of aggregate feedback. No improvement in compliance was observed during the intervention phase despite continued monitoring and dissemination of performance feedback.
CONCLUSIONS: Implementation of electronic hand hygiene monitoring with aggregate feedback was associated with a statistically significant decrease in compliance among resident physicians. These findings suggest that passive monitoring and group-level feedback alone may be insufficient to drive sustained behavior change. Additional strategies, including individualized feedback and behavioral interventions, may be necessary to improve adherence. Further research is needed to optimize implementation of electronic monitoring systems in graduate medical education settings.
Improving Clinic Cycle Time and Team-Based Efficiency Through Agenda Setting in an Ambulatory Resident Clinic
AUTHORS: Nancy Rodriguez, MD, MPH, MBA, MHA, Andrea Collingwood, DO, Autumn Johnson, MD, MS, Einav Silverstein, MD, Matthew Yu, DO, MPH, DipABLM, FAAFP, Karamjit Chela, MD, MPH
AFFILIATIONS: Department of Family Medicine at Charles R. Drew University of Medicine and Science, LAC-DHS Martin Luther King Jr. Outpatient Center
INTRODUCTION: Extended patient cycle time, defined as the interval from check-in to departure, is a persistent operational challenge in academic family medicine clinics, affecting patient satisfaction, staff overtime, faculty-resident morale, and the learning environment. At our institution, prolonged wait times, late-running sessions, and findings from a voluntary ACGME Special Review prompted a formal quality improvement initiative. Root-cause analysis identified incomplete resident agenda setting at visit onset as a modifiable upstream contributor to prolonged encounter and precepting times.
METHODS: This prospective observational quality improvement study examined three clinic cycles: Cycle 1 (January 2026), Cycle 2 (February 2026), and Cycle 3 (April–May 2026, post-intervention). Hand-recorded timestamps were collected at seven workflow transition points per visit. Subgroup analyses evaluated cycle time by clinic day/session, PGY year, attending preceptor, and individual resident. The intervention included a structured resident agenda-setting workshop, preceptor orientation, and Monday PM session redesign implemented in April 2026. This study serves as the objective outcome anchor for companion studies assessing faculty, nursing, patient, and resident perspectives.
RESULTS: Baseline data from Cycles 1 and 2 will be presented. Preliminary findings demonstrated mean total cycle times of 97–110 minutes, exceeding the 90-minute program target. Monday PM PGY-2 sessions were consistently the longest across both baseline cycles, with mean cycle times of 134–165 minutes. Preceptor-associated cycle times ranged from 82 to 149 minutes within the same residency program, suggesting substantial workflow variation by session structure and supervision patterns. Cycle 3 post-intervention data will be available at the time of presentation and will serve as the primary outcome measure.
CONCLUSIONS: Baseline findings demonstrate that prolonged cycle time in residency clinics reflects multiple structurally distinct and modifiable contributors rather than a single system-wide issue. Identifying specific sessions, preceptors, and training levels associated with the greatest inefficiency may provide more actionable targets for intervention than relying on program-wide averages alone. Post-intervention findings will determine whether agenda-setting training improves clinic flow and reduces variability across sessions.
Impact of a Longitudinal Educational Intervention on Family Medicine Residents’ Knowledge of Lifestyle Medicine: A Pre- and Post-Intervention Assessment
AUTHORS: Secilia Salem, MD, Derjung M. Tarn, MD, PhD and Daniel T. Lee, MD
AFFILIATIONS: UCLA Department of Family Medicine
INTRODUCTION: Lifestyle Medicine (LM) is an evidence-based discipline that uses therapeutic lifestyle interventions to prevent, treat, and reverse chronic disease. Despite growing evidence supporting its clinical effectiveness, formal LM education remains limited in many graduate medical education programs. Improving physician knowledge of LM principles may enhance patient counseling and preventive care. This study evaluated the effect of a longitudinal educational intervention on understanding of core LM concepts.
METHODS: We conducted a pre- and post-intervention study among all 12 first-year residents in the UCLA family medicine residency program. The intervention consisted of an hour-long didactic presentation on LM, an emailed handout, and five 10 minute presentations reviewing evidence-based LM interventions and clinical applications, occurring over a three month period. Participants completed pre- and post-intervention questionnaires assessing their knowledge about LM (familiarity with LM principles, prevention strategies, training pathways, and the six core pillars of LM). Paired t-tests were used to assess overall differences in knowledge.
RESULTS: Of 12 first-year residents 33% were male and 67% female. All attended at least one presentation and completed both assessments; none attended all presentations. Approximately 75% reported some prior knowledge of LM, with one participant indicating previous formal training. Baseline knowledge was variable, with pre-test scores ranging from 11 of 27 (41%) to 27 of 27 (100%) correct (mean 17 of 27 [63%] correct, SD 4.22). Following the educational sessions, post-test scores increased significantly to a mean score of 23 of 27 (85%) (SD=12; range 59%–100%; p<0.001). Improvements were most notable in questions related to the core pillars of LM and preventive applications. Identification of all six pillars of LM increased from 8% at baseline to 42% following the intervention.
CONCLUSIONS: A three-month longitudinal educational intervention significantly improved first-year resident physicians’ knowledge of LM principles. These findings provide preliminary support for the potential role of targeted instruction in addressing gaps in training related to preventive and lifestyle-based care. Integrating LM education into residency curricula may better prepare physicians to incorporate evidence-based lifestyle interventions into clinical practice and support chronic disease prevention and management.
Weaving Trauma-Informed Care and Storytelling to Improve Chronic Disease Self-Care Among Unhoused Women Living with Multimorbidity: The HEALthy Beginnings Intervention
AUTHORS: Benissa E. Salem, PhD, RN, MSN, PHN, CNL (1); Adey M. Nyamathi, PhD, FAAN (2); Barbara Riegel, PhD, RN, FPCNA, FHFSA, FAHA, FAAN (3); Lillian Gelberg, MD, MSPH (4); Melissa Y. Wei, MD, MS, MPH (4); Nicholas Jackson, PhD, MPH (4); Angelique Rubio, BS (4); Dana Rose Garfin, MA, PhD (5); Stephanie Covington, PhD, LCSW (6); Evelyn Vega, MPH (7); Andrea Loera, BS (1); Tori Prescott, BA (1); Jacob Salvanera (1); Soomin Son (1); Christina Abdishoo (8)
AFFILIATIONS: (1) Joe C. Wen School of Nursing, University of California, Los Angeles, CA; (2) Sue & Bill Gross School of Nursing, University of California, Irvine, CA, USA; (3) Center for Home Care Policy & Research, VNS Health, New York, NY; (4) David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA; (5) School of Public Health, University of California, Los Angeles, Los Angeles, CA, (6) Institute of Relational Development, Center for Gender and Justice, San Diego, CA; (7) Downtown Women’s Center, Los Angeles, CA; (8) University of California, Los Angeles, Los Angeles, CA
INTRODUCTION: Middle-aged and older unhoused women with multimorbidity (MAO-UW) face significant challenges navigating multimorbidity, yet tailored interventions are nonexistent. To address these gaps, HEALthy Beginnings (HB), a nurse-and community health worker-delivered 12-week intervention which integrates trauma-informed care (TIC) and chronic disease self-care was created. TIC supports safety and empowerment while character-driven, storytelling supports knowledge transmission, self-reflection, and positive behavior change. This presentation explains how TIC and storytelling are woven into HB to support feasibility and chronic disease self-care.
METHODS: HB was developed by integrating existing curricula with TIC principles and storytelling and then refined through multiple rounds of feedback with stakeholders. To integrate TIC into HB, TIC literature was reviewed and applied throughout the protocol. To create “Deidra’s story”, the lived experiences of MAO-UW were reflected upon, and an unfolding short story and companion workbook was developed. Using a theater-style testing approach with unhoused women, HB was later evaluated with high acceptability (≥ 4.67/5.0) and pilot tested using a mixed-method, quasi-experimental, prospective, single-arm, single-site study with MAO-UW. Descriptive statistics (means, frequencies, etc.) were used to analyze the data.
RESULTS: A total of 70 people were screened and 23 racially and ethnically diverse MAO-UW (mean=52.7+/-8.7 years) were enrolled in the study if they self-reported being ≥ 40 years, biologically female, currently unhoused (e.g., residing in a public or private shelter), with multimorbidity (≥ 2 chronic conditions), English-speaking, understood the screening, and were not hallucinating and/or intoxicated. Most participants self-reported being Black/African American (48%) and being housing insecure, with 91% continuously unhoused for ≥ 1 year and 74% who reported ≥ 4 episodes of homelessness in the past three years. Program retention was strong with 74% completing the HB intervention, and 78% completing the three-month follow-up.
CONCLUSIONS: Integrating TIC and storytelling is a complementary approach to improve chronic disease self-care to support MAO-UW navigating multimorbidity. From research training to implementation, TIC empowers MAO-UW, provides safety, trust, and peer support. Complementing this approach, “Deidra’s Story” helps MAO-UW identify with a woman with similar life experiences, validate their experiences, reflect on her journey and their own. Trauma-informed storytelling is successfully integrated into the HB curriculum and advances the science of chronic disease self-care for MAO-UW navigating multimorbidity.
Improving Clinic Cycle Time and Team-Based Efficiency Through Agenda Setting in an Ambulatory Resident Clinic: Faculty Perspectives
AUTHORS: Nancy Rodriguez, MD, MPH, MBA, MHA; Christopher Seawright, MD; Kimberly Doughty, MD, MPH; Abdullah Tirmizi, DO, MA; Brett Wilson, MD; Matthew Yu, DO, MPH, DipABLM, FAAFP; Karamjit Chela, MD, MPH
AFFILIATIONS: Department of Family Medicine at Charles R. Drew University of Medicine and Science, LAC-DHS Martin Luther King Jr. Outpatient Center
INTRODUCTION: Efficient ambulatory care delivery in family medicine residency training is complicated by the supervisory structure of graduate medical education. Attending preceptors must assess resident readiness, guide clinical decision-making, and maintain visit pacing within limited clinic time. Agenda setting the practice of eliciting and prioritizing patient concerns at visit onset is a foundational communication skill associated with fewer late-arising concerns and improved visit efficiency. Faculty perspectives provide a key measure of whether communication training translates into observable resident behavior change.
METHODS: This prospective pre/post survey study included attending family medicine preceptors (estimated n=10–14) who completed a locally developed Likert-scale instrument before a structured resident agenda-setting workshop (April 2026) and approximately two weeks post-intervention (late April–early May 2026). Four domains were assessed: completeness of resident presentations, ability to balance patient and provider concerns, integration of health promotion during time-limited visits, and overall perception of session pace and on-time completion. This is one of four companion QI studies evaluating the same intervention alongside resident self-assessment, nursing operational perspectives, patient experience, and objective cycle-time data.
RESULTS: Data collection is ongoing. Pre-intervention survey findings and baseline cycle-time data from two observed clinic weeks (January–February 2026) will be presented. Baseline observational data identified substantial preceptor-associated variation in session cycle time, ranging from 82 to 149 minutes across attending assignments. This variation persisted across both baseline observation periods despite differing resident rosters, suggesting workflow differences beyond learner composition alone. Post-intervention faculty survey results and comparative analyses will be available at the time of presentation.
CONCLUSIONS: Attending preceptors are uniquely positioned to detect changes in resident communication behaviors, prioritization skills, and visit structure from a supervisory perspective. Their perceptions provide a clinically meaningful measure of whether agenda-setting training results in observable behavioral change. If aligned with improvements in cycle-time and other stakeholder outcomes, these findings may support a scalable communication-focused quality improvement model for family medicine residency clinics.
Joshua Tree Room - Case Reports
The Chilling Effects of the Unknown: Calciphylaxis
AUTHORS: Alejandra S. Lopez, MD; Nathan Bui, D.O. Candidate; Yadira A. Arguelles, MD; Jose M. Urbina, MD; Nariman Almnini, MD; Alejandro Gonzalez Perez, MD; Verna Marquez, APD, MD; Carol Stewart-Hayostek, PD, MD
AFFILIATIONS: Clinica Sierra Vista/Rio Bravo Family Medicine Residency Program
INTRODUCTION: Calciphylaxis (calcific uremic arteriolopathy) is a rare, life-threatening vasculopathy characterized by medial calcification as well as dermal and subcutaneous arteriole occlusion. It leads to painful purpuric plaques resulting in ulceration, necrosis, and systemic infection. Sepsis is the leading cause of death in patients. [1][4] Female sex, obesity, diabetes, secondary hyperparathyroidism, vitamin K deficiency, corticosteroid use, hypoalbuminemia, and systemic inflammatory or autoimmune disorders are risk factors. [5] Calciphylaxis is at times a complication of kidney disease.
METHODS: A 51 year old woman with past medical history of Type II DM, hypertension, hyperlipidemia, CHF, and Stage V chronic kidney disease on dialysis M/W/F presented in the ED on 8/20/2025 for lower abdominal pain with 3 months of palpable raised bumps on the abdomen, right groin, and breast. Medications included calcium and iron. Ecchymosis in the lower abdomen, back, breast, pubic area, and right groin were noted. CT of abdomen/pelvis showed coronary artery calcifications. CMP was unremarkable except albumin 1.8 and Phosphorus 6.4. The patient was admitted for intractable abdominal pain, found to have calciphylaxis. Nephrology was consulted and recommended stopping calcium acetate and iron. Also, nephrology ordered sevelamer, sodium thiosulfate IV post-hemodialysis, and cinacalcet. Additionally, plastics, wound care, and palliative care were consulted. Patient was started on the proper treatment upon hospitalization, and was discharged shortly after. One week later, she was admitted at another hospital in Bakersfield, resumed treatment, and passed away soon after.
DISCUSSION: Calciphylaxis presents a challenge for many physicians. It is detected with close clinical suspicion, and it can be mistaken for panniculitis or necrotizing fasciitis. The incidence of calciphylaxis is 3.5 new cases/1000 patient-years in ESRD patients on chronic hemodialysis. The mortality rate is 30% at 6 months and 50% at 12 months[1][5]. Early recognition and treatment are key. [9] The treatment of calciphylaxis includes wound care, dermatology, plastics consult, sodium thiosulfate, vitamin K, and discontinuation of agents that worsens its proliferation, such as calcium and iron. Physicians should consider calciphylaxis whenever there are rashes, skin fissures, or painful nodules, especially in ESRD patients on dialysis.
Nodes of Uncertainty: Lupus in Disguise or Lymphoma in Plain Sight
AUTHORS: Fatima Maqsood, DO; Adolfo Aguilera, MD
AFFILIATIONS: Riverside University Health System/UC Riverside Family Medicine Residency Program
INTRODUCTION: Diffuse lymphadenopathy on its own is a non-specific symptom. Add in fevers, night sweats, and weight loss and malignancy is now high on the differential. These same symptoms are also associated with systemic lupus erythematosus (SLE). However, they are rarely the presenting symptoms in patients diagnosed with SLE. Here we present a case of a 20 year old female who presented with six months of diffuse lymphadenopathy along with weight loss, fevers, and night sweats and was ultimately diagnosed with SLE.
METHODS: A 20-year-old female with no past medical history presented to the ED with 48 pound weight loss over 6 months along with fevers, night sweats, and diffuse lymphadenopathy. Due to high concern for lymphoma, patient was admitted and lymph node biopsy was done. On hospital day 2, patient had a seizure. EEG was done showing frequent epileptiform discharges arising in the bifrontal regions and she was started on Keppra. Due to concern for possible CNS lymphoma, lumbar puncture was performed. With biopsy results pending and a broad differential in mind, autoimmune labs were obtained and resulted with positive ANA, elevated titer, low C3, C4. Preliminary read on lymph node biopsy showed reactive lymphoid hyperplasia not consistent with Hodgkin lymphoma. Rheumatology recommended steroids for possible SLE. Patient demonstrated clinical improvement on steroids. Final pathology read resulted with no evidence of leukemia/lymphoma. Patient was discharged on a steroid taper with rheumatology follow-up for management of SLE and possible neuropsychiatric syphilis given new onset seizure.
DISCUSSION: Fevers, weight loss, and night sweats are classic B symptoms raising alarm bells for possible lymphoma. Diffuse lymphadenopathy further raises suspicion for malignancy. All of the above symptoms are also seen in SLE. However, they are rarely the presenting symptoms of the disease. In the absence of a more classic presentation such as malar rash and joint pain, the aforementioned constellation of symptoms trigger a wide differential including malignancy and infectious etiologies. In such patients, rheumatologic etiologies should also be considered, particularly when initial workup for infection and malignancy is negative. SLE should be considered on the differential for diffuse lymphadenopathy to facilitate prompt diagnosis and treatment.
Morquio syndrome, or mucopolysaccharidosis type IV (MPS IV), is a rare lysosomal storage disorder
AUTHORS: Sevak Nersesyans, MD; Chidiebere Udechukwu, MD; Arthur Peter Yagubyan MD; Amanpreet Kaur, DO; Christianne G.Reyes, MD; Saira Dar, MD
AFFILIATIONS: Mission Community Hospital Department of Family Medicine
INTRODUCTION: Morquio syndrome (MPS IV) is a rare autosomal recessive lysosomal storage disorder causing defective keratan sulfate degradation—most often from N-acetylgalactosamine-6-sulfate sulfatase (MPS IVA) or less commonly beta-galactosidase (MPS IVB). It presents in early childhood with progressive skeletal dysplasia: short stature, spinal deformities, joint laxity, and dysostosis multiplex. Extra-skeletal issues include corneal clouding, hearing loss, airway obstruction, cardiac valve disease, hepatomegaly, and odontoid hypoplasia risking atlanto-axial instability and spinal cord compression.
METHODS: A 37-year-old man with Morquio syndrome (MPS IVA) and advanced multisystem disease, ventilator-dependent via tracheostomy, gastrostomy-fed, nonverbal but cognitively intact, and with multiple indwelling devices, presented after accidental nephrostomy tube dislodgement. He was tachycardic with fever and hypotension consistent with sepsis. Labs showed leukocytosis and a urinary source, and imaging revealed nephrolithiasis with hydronephrosis in complex renal anatomy. Despite fluids, antipyretics, and broad-spectrum antibiotics, he progressed to septic shock requiring vasopressors and ICU care. He developed multi-organ dysfunction including acute hypoxic respiratory failure, acute kidney injury, metabolic acidosis, and volume overload. Source control was limited by obstructive uropathy and anatomy. Cultures grew multidrug-resistant organisms including carbapenem-resistant Enterobacterales; therapy was started but shock remained refractory. Care was transitioned to comfort measures, and he died with family present in the ICU.
DISCUSSION: This case highlights the rapid progression and high mortality of urosepsis in a patient with Morquio syndrome (MPS IVA) complicated by severe anatomic abnormalities and chronic device dependence. Morquio syndrome is a lysosomal storage disorder marked by skeletal dysplasia, restrictive lung disease, and multisystem involvement with preserved cognition. In this patient, urologic abnormalities and nephrostomy dependence predisposed to infection. Tube dislodgement caused obstruction and infection with carbapenem-resistant Klebsiella pneumoniae, limiting treatment options. Despite antibiotics, he developed refractory septic shock, ARDS, kidney injury, and multi-organ failure, underscoring the importance of early source control and limits of care.
A Case of Polypharmacy Fatigue: From AKI to Dialysis in a Patient with Refractory Volume Overload and Infiltrative Cardiomyopathy
AUTHORS: Basiru Omisore MD; Karen Castaneda MD; Syed Hasan MD; Sheila Toro MD; Kim Kyung MD; Michael Ozoemena MD; Ejodakeme Okojie MD; Kenechukwu Nweke MD
AFFILIATIONS: Rio Bravo Family Medicine Residency Program, Clinica Sierra Vista, Kern Medical Center
INTRODUCTION: Medication non-adherence can lead to severe cardiovascular and renal complications. A 54-year-old male with hypertension, diabetes, and hyperlipidemia presented with hypertensive emergency, acute kidney injury, and refractory volume overload after stopping medications for two months. Echocardiography showed biventricular thickening, and proteinuria was nephrotic range. He required hemodialysis despite diuresis. This case highlights the impact of non-adherence and the need for adherence-focused strategies.
METHODS: A 54-year-old male with hypertension, hyperlipidemia, and type 2 diabetes mellitus presented with progressive bilateral leg swelling, dyspnea, orthopnea, and urinary retention over two weeks. He admitted discontinuing all medications for two months due to polypharmacy fatigue. On admission, blood pressure was markedly elevated with evidence of hypertensive emergency. Laboratory studies showed acute kidney injury with elevated creatinine, reduced eGFR, and elevated BNP consistent with volume overload. Imaging revealed pulmonary congestion. Echocardiography demonstrated biventricular thickening suggestive of infiltrative cardiomyopathy. Urine studies showed nephrotic-range proteinuria. Bone marrow biopsy excluded plasma cell disorders. Despite aggressive intravenous diuresis, the patient developed refractory fluid overload requiring initiation of hemodialysis. Clinical status stabilized with dialysis and supportive care, and plans for close outpatient follow-up were arranged.
DISCUSSION: This case highlights the consequences of medication non-adherence in chronic cardiovascular disease. Discontinuation of antihypertensives and diuretics led to hypertensive emergency, acute kidney injury, and severe volume overload requiring dialysis. Polypharmacy fatigue is a key contributor to non-adherence, particularly in patients with multiple comorbidities. Biventricular thickening and nephrotic-range proteinuria further complicated management, suggesting underlying structural and renal disease. Early adherence could have prevented progression to end-organ damage. Strategies such as simplified regimens, combination therapy, and patient-centered education are essential to improve adherence and reduce morbidity.
Progressive Microcytosis, Hypochromia, and Thrombocytosis as Early Indicators of Gastric Adenocarcinoma: A Longitudinal Case Study
AUTHORS: Basiru Omisore MD; Karen Castaneda MD; Sheila Toro MD; Syed Hasan MD; Kim Kyung MD; Ebenezer Dadzie MD; Michael Ozoemena MD; Ejodakeme Okojie MD; Kenechukwu Nweke MD
AFFILIATIONS: Rio Bravo Family Medicine Residency Program; Clinica Sierra Vista; Kern Medical Center
INTRODUCTION: Subclinical iron deficiency may precede overt anemia and signal underlying malignancy. A 62-year-old male with diabetes presented with fatigue and was found to have severe anemia, progressive microcytosis, hypochromia, and thrombocytosis. Iron studies confirmed deficiency. Endoscopy revealed an ulcerated gastric mass, and biopsy confirmed adenocarcinoma. This case highlights the importance of recognizing hematologic trends as early indicators of occult gastric cancer.
METHODS: A 62-year-old male with type 2 diabetes, hypertension, and hyperlipidemia presented with fatigue, dizziness, and weakness. He reported epigastric discomfort, dark emesis, and melena. Prior labs showed progressive microcytosis and thrombocytosis. On admission, hemoglobin was 6.8 g/dL. Iron studies revealed low serum iron, low ferritin, and elevated total iron-binding capacity, consistent with iron deficiency anemia. Physical exam showed pallor and mild epigastric tenderness. He received two units of packed red blood cells. Endoscopy demonstrated a large ulcerated gastric mass involving the antrum and body. Biopsy confirmed invasive poorly differentiated gastric adenocarcinoma. The patient was stabilized and discharged with follow-up for oncologic evaluation and management.
DISCUSSION: This case demonstrates that progressive microcytosis, hypochromia, thrombocytosis, and iron deficiency may precede symptomatic gastric cancer. These hematologic changes reflect chronic occult blood loss and inflammation. Microcytosis, even without severe anemia, can signal increased cancer risk, while thrombocytosis may represent a paraneoplastic response. In patients with comorbidities, these findings may be overlooked or attributed to chronic disease. Early recognition of laboratory trends could prompt timely evaluation and diagnosis before advanced disease develops. Integrating longitudinal hematologic data into routine care is critical for early detection.
Not The Leg, Too!
AUTHORS: Layla Nejad, MD and Bernadette Pendergraph, MD
AFFILIATIONS: Department of Family Medicine at Harbor-UCLA
INTRODUCTION: Lateral ankle sprains are among the most common injuries evaluated in primary care. With clinical tools such as the Ottawa Ankle Rules limiting unnecessary imaging, inability to bear weight remains an important indication for further evaluation. A 41-year-old male with a mechanism consistent with a lateral ankle sprain required advanced imaging because of his inability to take 4 steps. Despite no reported history or recollection of prior injury, imaging revealed both acute and chronic fibular injury, highlighting the importance of a thorough lower extremity exam to avoid missed diagnoses.
METHODS: A 41-year-old male was evaluated by his PCP after two ED visits for persistent pain after a left ankle inversion injury from football. Initial radiographs were negative, and he was discharged in an ACE wrap with crutches and NSAIDs. Concerned for a syndesmosis injury, the PCP ordered an MRI, placed him in a CAM boot, and referred him to sports medicine. On exam, there was anterolateral ankle swelling and ecchymosis with limited range of motion. Tenderness was noted over anterior talofibular ligament (ATFL), anterior tibiofibular ligament, distal syndesmosis, posterior tibial tendon, and 13-21 cm above the distal tip of the fibula. He had 2+ anterior drawer and negative tib-fib compression test. Repeat ankle x-rays remained negative, but tib-fib x-ray showed an old midshaft fracture with lucency. MRI confirmed ATFL tear and medial ankle flexor tendinitis. He was diagnosed with a lateral ankle sprain and a midshaft fibular fracture, treated with a long leg walking boot for 6 weeks followed by a course of physical therapy.
DISCUSSION: Midshaft fibular fractures usually occur from direct trauma in sports and are often treated nonoperatively. Interestingly in this case, the athlete did not recall prior trauma to his leg, yet imaging revealed both a prior healed midshaft fibular fracture and a new fracture supported by an area of lucency. Ankle sprains associated with mid-shaft fibular fractures are commonly associated with unstable ankle injuries involving the syndesmosis or deltoid ligament. However, the athlete’s weight bearing radiographs demonstrated a stable syndesmosis. This case highlights the importance of a comprehensive exam with palpation proximal to the ankle, as a Maisonneuve fracture, a fracture involving the proximal fibula with an unstable ankle injury, is an important “not miss” diagnosis.
Moyamoya Disease, a Formidable Etiology of Cerebrovascular Ischemia
AUTHORS: Sabbah Georgette MD; McLaughlin Nathan MD
AFFILIATIONS: Riverside University Health System
INTRODUCTION: Cerebrovascular accidents can occur from a genetic mutation not considered to be a leading differential diagnosis upon presentation. Moyamoya disease is a rare cerebrovascular disease characterized by progressive stenosis of the internal carotid artery and its main branches, resulting in fragile collateral vessels at the base of the brain termed moyamoya vessels. Approximately 0.29 percent of the United States population was affected by Moyamoya disease in 2024. The infrequency with which it is encountered makes it a rare etiology of cerebrovascular ischemia worthy of further investigation.
METHODS: A 40-year-old right-handed female with past medical history of cerebrovascular accident with residual deficit of dysarthria, type 2 diabetes mellitus, hypertension, and gallstone pancreatitis presented with persistent right-sided body tingling for one month. CT Head and CT Angiogram of the Neck performed were negative for acute intracranial pathology. However, they were evident for chronic infarcts in the right inferolateral parietal lobe and left anterior basal ganglia. CT Angiogram of the Head noted bilateral M1 stenosis with concern for possible Moyamoya syndrome. As a result, Neuro-interventional Radiology was consulted and completed a diagnostic cerebral angiogram, which showed advanced moyamoya changes compatible with advanced Moyamoya disease. In response, Neurosurgery was consulted to evaluate for possible surgical intervention, such as Extracranial to Intracranial and Superior Temporal Artery to Middle Cerebral Artery bypass. However, no surgical intervention was recommended. Neurology recommended initiation of Cilostazol and to continue high-intensity statin therapy.
DISCUSSION: This case illustrates an alternative etiology of cerebrovascular accident that is not commonly considered a differential diagnosis, and the value of imaging in assisting with accurate diagnosis. Although the source of ischemia in this case is rare, it can present in both pediatric and adult populations, with peak incidence at approximately five and forty years old. Once identified, surgical revascularization should be considered immediately to establish collateral pathways, as it is the first-line treatment. Unfortunately, there are no effective medical therapies for the acute management of Moyamoya disease, making early clinical recognition essential. Preventative measures include management of stroke risk factors, analgesics for headaches, and antiepileptic agents for seizure management.
Direct Initiation of Long-Acting Injectable Buprenorphine in a Patient with opioid use disorder: A Case Report
AUTHORS: Muhammad Safwatullah, MD, MPH; Matthew Beare, MD; Milagros Becerra Ramirez, MD;, Isabello Lucho Bustamante, MD; Abel Rojas- Parra, MD
AFFILIATIONS: Addiction Medicine Fellowship Program, Clinica Sierra Vista, Bakersfield, CA
INTRODUCTION: From 1999–2023, about 806,000 people died from opioid overdoses in the U.S. Buprenorphine, a partial μ-opioid receptor agonist, is a cornerstone FDA-approved treatment for opioid use disorder that reduces cravings, withdrawal, and all- cause and overdose mortality with lower respiratory risk than full agonists. However, initiating it can be challenging due to its high receptor affinity which can precipitate withdrawal if started too early. Standard inductions require moderate withdrawal, while alternatives like micro-dosing can be complex, calling for practical and patient-centered approaches.
METHODS: We present a patient with severe opioid use disorder and daily fentanyl use via smoking who presented for buprenorphine initiation. After counseling on various induction methods, patient chose a direct-to-injection approach with long-acting buprenorphine, a novel strategy that does not require a period of abstinence. Adjunctive medications prescribed were ondansetron, clonidine, ibuprofen, hydroxyzine, and oral rehydration solution. Induction comprised of three consecutive daily injections with 2nd Generation long-acting buprenorphine. However, due to logistics, the third dose occurred on day 4 as follows: day 1, weekly 8 mg; day 2, weekly 16 mg; day 4, monthly 128 mg. The patient was seen four times during induction. Success was assessed by Clinical Opiate Withdrawal Scale (COWS) scores and continued engagement. He experienced no precipitated withdrawal and remained clinically stable. He reported good tolerability as follows: day 1,COWS 0 (last fentanyl use ~2 hours prior); day 2, COWS 2 (last use ~1 hour prior); day 4, COWS 4 (last use ~2 hours prior).
DISCUSSION: This case shows transition from fentanyl to buprenorphine using a direct-to-injection which was first described in ED-INNOVATION trials and related studies including Water et al. Unlike traditional methods, this novel method does not require abstinence, as the initial weekly formulation rises slowly in the system and peaks around 24 hours thereby reducing precipitated withdrawal risk. By day 2, buprenorphine increasingly displaces fentanyl at opioid receptors, with the subsequent weekly 16 mg dose further increasing receptor occupancy. Administration of the 128 mg monthly dose then achieves cravings and withdrawal symptoms for the rest of the month. Overall, this stepwise approach provided a smooth transition avoiding precipitated withdrawals.
The Airway You Can’t Ignore: Impending Obstruction from a Neck Mass in Clinic
AUTHORS: Einav Silverstein, MD; Matthew Yu, DO, MPH
AFFILIATIONS: Charles R. Drew University Family Medicine Residency Program
INTRODUCTION: Central airway obstruction (CAO), generally defined as >=50% central airway occlusion, is a life-threatening emergency that demands rapid recognition before complete obstruction occurs. In the outpatient setting, identifying early warning signs is a critical and underemphasized skill. We present an 80-year-old male with bilateral neck masses, episodic self-resolving dyspnea, and profound weight loss whose outpatient encounter prompted emergent referral, ultimately revealing diffuse large B-cell lymphoma with impending CAO requiring urgent tracheostomy.
METHODS: An 80-year-old male with a decades-long smoking history presented to an outpatient urgent care clinic with a 6-week history of progressive bilateral neck masses and 45-pound unintentional weight loss. He reported several self-resolving episodes of dyspnea lasting several seconds over the preceding days. Examination revealed a grapefruit-sized, fixed, nontender right submandibular mass with left cervical adenopathy, audibly noisy breathing at rest, and visible tumor invasion of the soft palate and lateral pharynx. The patient was urgently referred to the emergency department for airway monitoring and ENT consultation. CT neck demonstrated bilateral necrotic cervical nodal conglomerates, and flexible nasolaryngoscopy confirmed a hypopharyngeal mass with obstructed view of the glottis. He was admitted to the ICU for airway watch, and urgent tracheostomy was performed the following day to relieve compressive symptoms on airway. Biopsy confirmed diffuse large B-cell lymphoma with BCL6 rearrangement.
DISCUSSION: This case illustrates that even in the absence of acute respiratory distress, it is important to recognize key outpatient red flags for impending CAO including voice changes, noisy breathing at rest, intermittent and/or positional stridor/stertor/wheezing, bulky neck masses, and visible pharyngeal invasion. Though symptoms may initially be subtle, such patients can decompensate very quickly and require emergent CT imaging, ENT consultation, and ICU-level airway monitoring as soon as possible upon recognition. It is imperative that family physicians, as first-contact providers, become comfortable identifying these warning signs before complete obstruction occurs to be able to direct escalation of care appropriately.
Ertanercept in Reactive Infectious Mucocutaneous Eruption
AUTHORS: Thomas Bird, MBBS, Nina Fukuma, MD, Patricia Ruano, MD, Justin So, MD, Tara Thacker, MD
AFFILIATIONS: Kaiser Permanente Los Angeles Medical Center, Family Medicine
INTRODUCTION: Reactive infective mucocutaneous eruption (RIME) is characterized by mucositis involving the oral, ocular, and urogenital mucosa in the setting of an infectious trigger, most commonly Mycoplasma pneumoniae. While most cases occur in the pediatric population, RIME also affects young adults and poses diagnostic challenges due to overlap with Stevens-Johnson syndrome, Behçet disease, and other causes of mucositis. We present the case of a patient who developed severe mucositis in the setting of M. pneumoniae infection, diagnosed as RIME and successfully treated with azithromycin and etanercept.
METHODS: 27 year old female, with history of HSV-1, presented to the ED with fevers, cough, nasal congestion, and sore throat in the setting of recent travel to Indio, CA. Following empiric treatment with amoxicillin and azithromycin, patient presented to the ED on day 12 of symptoms, now with severe bilateral blepharoconjunctivitis with subconjunctival hemorrhage as well as conjunctival, oral, and genital mucositis. Work up was notable for positive Coccidiomycoses IgM, but negative IgG, suggesting a false positive, as well as negative HIV, syphilis, HSV, VZV, murine typhus IgG, and RPP. Patient’s autoimmune work up, including ANA, ANCA, dsDNA, HLAB51, and pathergy test, returned negative, making Behchet’s syndrome less likely. Infectious work up was notable for positive Mycoplasma IgM (2.32; normal <0.76), suggestive of a highly significant amount of M. pneumoniae antibody. The patient was evaluated by dermatology, ophthalmology, and rheumatology, and found to have RIME. Following treatment with Azithromycin and Etanercept, patient had significant improvement to symptoms.
DISCUSSION: RIME is uncommon, seen in only 11-13% of patients hospitalized for M. pneumoniae, and more often in pediatric patients (1,2). Given the broad differential for rashes following a viral prodrome, it is important to bring light to RIME to ensure accurate diagnosis and treatment. The mucositis seen in RIME may be mistaken for SJS/TEN or Behcet’s, and the viral prodrome may also be confused for Hand-Foot-Mouth (3). While there are no consensus guidelines for RIME, studies demonstrate that serology for Mycoplasma pneumoniae, as used inour case, may offer greater clinical utility than PCR by capturing both current and recent infections (4).
Pigmented Villonodular Synovitis: A Recurrent Knee Effusion
AUTHORS: Daniel Zumerkorn Hassan, MD; Yuntao Dai, MD, PhD; Arthur Peter Yagubyan, MD; Steven Narvy, MD, Petros Hajian, DO
AFFILIATIONS: Mission Community Hospital, Department of Family Medicine, Los Angeles, CA; LA Bone and Joint Institute, Department of Sports Medicine, Los Angeles, CA
INTRODUCTION: Pigmented villonodular synovitis (PVNS) is an uncommon synovial disorder that remains a diagnostic challenge due to its insidious onset and nonspecific presentation. It typically affects a single joint, knee or hip, and presents with slowly progressive pain and swelling. Physical examination may be unremarkable, and initial radiographs are often normal. Magnetic resonance imaging (MRI) characteristically demonstrates joint effusion, synovial hypertrophy, capsular distension, and low signal intensity due to hemosiderin deposition.
METHODS: A 25-year-old female with no significant past medical history presented to a sports medicine clinic with knee pain, swelling, and a recurrent knee effusion persisting for approximately three months. Physical examination revealed persistent knee edema with recurrent effusions. The patient experienced only transient symptom relief following prior interventions, with rapid recurrence of swelling. The patient initially received an injection during an emergency department visit, followed by an orthopedic evaluation with intra-articular corticosteroid injection. Despite these treatments, symptoms persisted. Knee aspiration performed during visit yielded approximately 25 mL of yellow synovial fluid. Given recurrent effusions and failure of conservative management, MRI of the knee was obtained, revealing synovial proliferation with characteristic findings consistent with PVNS. The patient was referred to orthopedic surgery for evaluation and management.
DISCUSSION: This case highlights the importance of early MRI evaluation in patients with recurrent knee effusions unresponsive to aspiration and injection to avoid diagnostic delay and unnecessary procedures.
Lectern Session 1 (1:40 – 2:25PM)
Vitamin B12 Screening and Deficiency in Type 2 Diabetes Mellitus Patients on Metformin
AUTHORS: Tyler Goldberg, MD, PharmD (1), Lilit Balian, PharmD (2), Monique George, MD, FAAFP (1), Kimi Pontoppidan, PharmD, APh (2), Hasmig Ekmekdjian, PharmD, APh (2)
AFFILIATIONS: (1) Kaiser Permanente Woodland Hills Family Medicine Residency Program; (2) Kaiser Permanente Woodland Hills Pharmacy Residency Program
INTRODUCTION: Metformin is a first-line therapy for the management of Type 2 Diabetes Mellitus (T2DM). The American Diabetes Association (ADA) acknowledges that long-term metformin use may lead to vitamin B12 deficiency. However, no universally accepted screening guidelines exist. Timely assessment supports cost-effective, preventive care by identifying a reversible cause of anemia, neuropathy, and cognitive decline before irreversible harm occurs. This study evaluates metformin-associated vitamin B12 deficiency and aims to close gaps in clinical practice through standardized screening recommendations that promote earlier detection and intervention.
METHODS: This is a retrospective observational cohort study conducted within the Kaiser Permanente Southern California (KPSC) region. Data was extracted from Kaiser Permanente’s electronic health record (EHR between January 1, 2014, and December 31, 2024. Factors collected included age, sex, race, total daily metformin dose, duration of metformin therapy, proton pump inhibitor (PPI) use, and vitamin B12 testing and serum values. Primary endpoints evaluated the rate (%) of vitamin B12 deficiency screening and the prevalence of vitamin B12 deficiency (less than or equal to 200pg/mL). Secondary endpoints assessed the association between metformin dose (mg/day) and duration of metformin therapy, with vitamin B12 deficiency. Comparative analyses were conducted using Chi-Square and T tests.
RESULTS: The pertinent inclusion criteria were metformin use of at least 1000mg/day and a diagnosis of T2DM. The exclusion criteria were Type 1 Diabetes Mellitus, prior vitamin B12 deficiency, anemia, alcoholism, history of gastric bypass, HIV, pregnancy, celiac disease, Chron’s disease, ulcerative colitis, immunosuppressive therapy, and active cancer. Given these parameters, 136,913 subjects were included in the study. Of the sample size, ~32% of patients were ordered for Vitamin B12 testing, of which ~29% completed testing and ~5% were found to be deficient. Particularly for the subjects using 2000mg/day or more, there was a positive correlation between dose and vitamin B12 deficiency (6%; P<0.0001), as well as deficiency rate and duration of therapy (5% deficiency rate at 48 months; P=0.0113).
CONCLUSIONS: The observational data shows a statistically significant relationship between metformin dose, particularly 2000mg/day and above, and vitamin B12 deficiency, less than or equal to 200pg/mL. There is also a statistically significant relationship between duration of therapy, particularly above 2 years, and vitamin B12 deficiency. However, only ~32% of the study population were offered Vitamin B12 testing. Therefore, providers may consider annual vitamin B12 testing in patients with T2DM receiving metformin therapy, especially higher doses, and particularly if treated for 3 years or more.
Enhancing Early Autism Detection: Implementing M-CHAT R/F Screening in a Primary Care Clinic in Panorama City, CA
AUTHORS: Natalia Henriquez, MD; Sabrina Afroz, MD; Lauren Joseph, MD
AFFILIATIONS: Mission Community Hospital, Department of Family Medicine
INTRODUCTION: Autism spectrum disorder affects 1 in 36 children in the United States, yet early detection remains inconsistent in primary care. Validated tools such as the Modified Checklist for Autism in Toddlers, Revised with Follow-up (M-CHAT-R/F) improve early identification and outcomes. However, screening adherence during well child checks is often suboptimal. This project aimed to implement a standardized M-CHAT R/F protocol for children during Well Child Checks (WCC) at 18, 24, and 30 months at the Santo Nino Health Clinic (SNHC) in Panorama City, CA.
METHODS: This quality improvement study was conducted at a primary care clinic in Panorama City, California. Interventions began January 2025 and included resident education, front desk distribution of screening forms at 18- and 24-month visits, and catch-up screening at 30 months. Additional measures included electronic medical record alerts, provider reminders, and follow-up communications. Data from pediatric encounters (ages 1–4) between October 2024 and February 2026 were reviewed; 80 met inclusion criteria. Screening compliance rates were analyzed using a statistical process control P-chart to assess changes over time.
RESULTS: Baseline screening compliance was 12.5% from October to December 2024. Following implementation of interventions, compliance demonstrated a sustained increase. The overall average screening rate rose to 39%, with a peak of 75% observed between June and August 2025 after full intervention deployment. Although values remained within control limits, the upward shift indicates improved adherence to screening practices. No significant adverse workflow disruptions were reported during implementation.
CONCLUSIONS: A structured, multi-component intervention significantly improved M-CHAT-R/F screening rates in a primary care setting. Key drivers included provider education, electronic medical record integration, and workflow optimization. These findings support scalable strategies to enhance early autism detection and reinforce the role of primary care in timely diagnosis and referral for developmental services.
From Crisis to Care: How Medication-Assisted Therapy (MAT) Reduces Emergency Department (ED) Visits in Opioid Use Disorder (OUD) – An Expanded Analysis of a Growing MAT Program
AUTHORS: Fatima Maqsood, DO; Pavan Anand, MD; Esther Zarecki, MD; Faheem Jukaku, MD; Raymond Kramer, MD
AFFILIATIONS: Riverside University Health System/UC Riverside Family Medicine Residency Program
INTRODUCTION: Over 1 million have died from drug overdose since 1999 with overdose from opioids making up 76% of those deaths. Increased availability of treatment has led to a 13-27% decrease in overdose fatalities. Unfortunately, most patients do not receive OUD treatment due to low adoption rates of MAT by providers. In this study, we aim to quantify the impact of MAT for patients with OUD in a single clinic in Riverside County as the MAT program expands and more patients are inducted into treatment. We hypothesize that patients who seek and regularly receive MAT due to OUD have a reduction in ED visits compared to those with OUD who do not receive MAT.
METHODS: This is a retrospective study looking at the effectiveness of MAT in patients diagnosed with OUD in a single clinic in Riverside County between 2019, when MAT services initiated, to 2026. We hypothesized that patients diagnosed with OUD with MAT services would have decreased ED usage. Inclusion criteria are patients who are at least age 18 with diagnosis of OUD. The primary outcome was a reduction in ED visits. A Wilcoxon signed-rank test was used to compare the number of ED visits 1 year before and 1 year after MAT clinic initiation. Outliers were excluded using the interquartile range (IQR) method. A p-value < 0.05 was considered statistically significant.
RESULTS: A total of 203 patients were analyzed, with 21 patients being classified as outliers. Therefore, 182 patients who established care at the MAT clinic prior to March 2025 and had complete ED visit data were included in the analysis. The mean number of ED visits decreased from 1.687 before MAT to 1.157 after MAT, yielding a mean reduction of 0.53 visits. A Wilcoxon signed-rank test showed this reduction was statistically significant (p < 0.0001). Among patients with more than 3 MAT visits (n = 161), the reduction was also significant (mean = 0.453 visits, p = 0.0001). These findings support the efficacy of MAT in reducing ED visits.
CONCLUSIONS: OUD continues to drive high rates of ED utilization due to medical complications and lack of consistent care. Our findings add to evidence that MAT reduces acute care needs. Even in a small community setting, MAT led to meaningful ED reductions—especially for those with >3 visits, highlighting the value of continuity. The MAT clinic’s dual role as primary care may have improved access and outcomes. Our expanded results continue to show promise regarding the efficacy of MAT programs. Larger studies and further analysis can assess potential confounding variables and guide implementation.
Retrospective Cohort Study Comparing Corticosteroid to PRP and PRP Plus Corticosteroid Injection to Time to Knee Replacement in Individuals with Knee Osteoarthritis in Kaiser Permanente Southern California
AUTHORS: Jacqueline Sandoval DO MS, Michael Fong MD CAQSM, Nick Hu MD, Debbie Meskin DO, Cody Webb MD, Stacee Horwitz MD, SeungYong Han PhD
AFFILIATIONS: Kaiser Permanente Los Angeles - Sports Medicine
INTRODUCTION: Knee osteoarthritis (OA) is highly prevalent in the United States. Corticosteroid (CS) injections offer short-term symptom relief after conservative therapy but carry risks and may not provide durable benefit. Platelet-rich plasma (PRP) has emerged as an alternative, with evidence of pain and functional improvement lasting up to 12 months. However, no studies have evaluated whether PRP affects the time from initial injection to knee replacement surgery.
METHODS: This retrospective cohort study used Kaiser Permanente Southern California data from January 2016 to February 2024. Adult patients with Kellgren–Lawrence grade 0-4 knee OA who received CS only, PRP only, and PRP + CS injections were identified through ICD-10 and CPT codes. Covariates included age, sex, BMI, race/ethnicity, and Elixhauser comorbidity score. Time to knee replacement was analyzed using a Cox proportional hazards model.
RESULTS: Compared with CS, neither PRP (HR 0.713; 95% CI: 0.356–1.432; p=0.342) nor PRP+CS (HR 1.152; 95% CI: 0.973–1.364; p=0.102) significantly affected time to knee replacement. Higher BMI (overweight HR 1.375; 95% CI: 1.307–1.446; obese HR 1.362; 95% CI: 1.298–1.430) and older age (60–69 HR 1.875; 95% CI: 1.809–1.944; ≥70 HR 1.667; 95% CI: 1.602–1.734) increased hazard. Female sex was associated with lower hazard (HR 0.964; 95% CI: 0.936–0.993; p=0.014). White patients had higher hazard (HR 1.262; 95% CI: 1.222–1.304), while other groups had lower hazard (HR 0.942; 95% CI: 0.903–0.982) in comparison to Hispanic patients. Higher Elixhauser score was associated with lower hazard (HR 0.981; 95% CI: 0.978–0.983), likely reflecting selection bias.
CONCLUSIONS: PRP, alone or combined with CS, was not associated with delayed knee replacement compared with CS alone. Strong associations were observed for BMI, age, race/ethnicity, and sex as comorbidity burden. The small PRP sample size may have limited the ability to detect differences. Future studies should compare PRP cohort and PRP + CS cohort with adequate sample sizes in order to explore the role of BMI, age, race/ethnicity, and sex in modifying progression to knee replacement.
Poster Session 2 (2:25 – 3:05PM)
Cabrillo Room - Abstracts
Development of the Home Care Worker Working Conditions Survey
AUTHORS: Ricardo Antillon, MPH, Geoffrey Gusoff, MD, MS, MBA
AFFILIATIONS: UCLA Department of Family Medicine
INTRODUCTION: Home care is a growing job sector which tries to meet the demands of the growing older adult population and others who require assistance to live comfortably in their home. Although this job is in such high demand, and of such high importance, the home care workforce is marked by high turnover and low job satisfaction. Home care cooperatives, agencies co-owned by their workers, report half the worker turnover of traditional agencies. To understand what workplace factors are most strongly associated with workforce turnover at cooperatives and traditional agencies, we developed the Home Care Worker (HCW) Working Conditions Survey instrument.
METHODS: The first step in our instrument development was to do a thorough literature review to identify currently available working conditions instruments that are HCW specific, or general working conditions instruments which align well with HCWs. We then utilized a RAND-inspired Delphi review method where experts ranked survey items by importance to then develop the first survey draft. English cognitive interviews were conducted to refine items for understandability among HCWs. This finalized the first survey draft, which was used for a pilot study that surveyed cooperative and non-cooperative caregivers. Based on pilot study data, the English survey was finalized, translated into Spanish, and Spanish cognitive interviews were conducted to refine items for clarity among Spanish-speaking HCWs.
RESULTS: Through the literature review, we identified 729 potential survey items. These items were then organized among 11 domains, and presented to a panel of 8 experts. These experts went through the survey items and graded them from a scale of 1 to 10. Based on item grading, 120 survey items were chosen for the initial survey instrument. Twenty-seven cognitive interviews were conducted to refine the instrument for better understanding amongst HCWs. The refined survey draft was then used in a pilot study of 100 caregivers. The items were then psychometrically evaluated to further reduce the instrument to 90 items.
CONCLUSIONS: The final 90 item survey is currently being administered to various cooperative and non-cooperative home care agencies, with the aim of collecting 1000 HCW responses. Once data collection is complete, the next steps are to psychometrically analyze the data to determine if it follows the same trends seen during the pilot study. Further refinement of the survey will enable researchers and practitioners to more reliably evaluate home care working conditions and their relationship to turnover and job satisfaction.
A Needs Assessment to Characterize the Social Priorities at a Clinic for Unhoused Individuals
AUTHORS: Gladys Bello, BS (1); Jacqueline Cabral, BA (1); Alejandra Rivas, BA (1); Erika Venegas,BS (1); Joselyne Camacho, BA (2); Leonor Georgette Farias, BS (2); Jyoti Puvvula, MD, MPH (2); Gilberto Granados, MD, MPH (2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA, PRIME-LA, Los Angeles, CA; (2) Harbor UCLA Department of Family Medicine
INTRODUCTION: At a free clinic in Los Angeles, over half of patients reported anxiety or depression, yet only one requested mental health services. This paradox reflects a broader challenge: healthcare systems often offer what they can provide rather than centering on what patients are in need of most. Among individuals experiencing homelessness, social conditions frequently compete with clinical concerns as daily priorities. This study characterizes patient-identified assistance needs at a free clinic to better understand how service offerings align with the lived priorities of patients experiencing homelessness.
METHODS: Cross-sectional needs assessment at Redondo Beach Free Clinic, a Harbor-UCLA Family Medicine-operated clinic serving individuals experiencing housing insecurity in the South Bay of Los Angeles County. Data were collected from March 2023 through October 2024 (N=46). Surveys assessed demographics, housing status, insurance coverage, self-reported health conditions, healthcare utilization in the prior six months, and patient-identified assistance needs across nine domains, including housing, dental care, transportation, food access, employment, education, mental health services, and insurance enrollment. Descriptive statistics were calculated using pairwise deletion for missing responses.
RESULTS: Of 46 participants, 72% were male, 85% unemployed, and 57% unsheltered. Patient-identified priorities were predominantly social: housing (71%, n=30/42), dental care (67%, n=28/42), transportation (57%, n=24/42), and food access (55%, n=23/42). Employment and education were cited by 45% and 40%, respectively. Notably, 51% reported anxiety or depression, yet only 28% (n=12/42) identified mental health services as a priority. Seventy-four percent (n=32/43) had health insurance; however, 53% of insured participants lacked a primary care clinician, and most had not accessed dental (70%) or vision care (76%) in the prior six months. Clinical services did not rank among patients' top four stated priorities.
CONCLUSIONS: Patients experiencing homelessness identify social determinants as their most pressing priorities, despite having insurance coverage and a significant mental health burden. These findings present an opportunity to align services with patient-expressed needs through social needs screening and community referrals. In response, we partnered with UCLA Luskin MSW students to implement patient navigation services targeting basic needs assistance, insurance enrollment, primary care linkage, specialty referrals, and transportation services. Future evaluation will assess the impact on care utilization.
Anesthesiology Resident Preparedness for Older Adult Care
AUTHORS: Gustavo Castellanos, BS (1); Cecilia Canales, MD, MPH (1)(2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA; (2) UCLA Health Department of Anesthesia
INTRODUCTION: In the U.S., 5 million older adults undergo surgery annually. Older adults have the highest prevalence of surgery and face disproportionate risk of perioperative neurocognitive disorders. The American Society of Anesthesiologists (ASA) recommends routine cognitive and frailty screening, evidence-based intraoperative pharmacologic strategies, and postoperative delirium assessment to improve outcomes. However, adherence remains limited. We hypothesized that anesthesiology residents would report low confidence in performing geriatric assessments and applying perioperative best practices.
METHODS: We conducted a cross-sectional needs assessment of anesthesiology residents (CA-1 to CA-3) at a large academic medical center. The instrument was developed from the ASA and American Geriatrics Society guidelines. Three geriatric anesthesia experts reviewed for content validity, and face validity was established with 15 graduating residents. Domains included preoperative risk stratification, intra/postoperative management, and self-reported preparedness to care for older adults. Responses used a 5-point Likert scale, and descriptive statistics were applied.
RESULTS: Of 81 residents, 65 responded (80.2%), [CA-1: n=23; CA-2: n=25; CA-3: n=17]. 94% reported caring for older adults "daily" or "several times per week.” Despite this, residents reported significant deficits in geriatric competencies. 100% reported low confidence (Likert score 1-2) to perform validated frailty assessments, and 77% reported low confidence in administering cognitive screening tools. While residents expressed higher confidence in physiologic management, confidence was significantly lower for delirium screening and application of results to clinical care. 56% disagreed or strongly disagreed that they had received formal didactic instruction in perioperative geriatric medicine.
CONCLUSIONS: Anesthesiology trainees report high exposure to older adult surgical care but feel unprepared to apply evidence-based geriatric anesthesia practices. These findings support the need for structured, competency-based curricula in geriatric anesthesia.
An Innovative Chaplain-Integrated Wound Care Delivery Model for the Streets of Skid Row: A Mixed-Methods QI Evaluation
AUTHORS: Cindy Curiel; Gerardo Moreno, MD MS; and Mary Marfisee, MD, MPH
AFFILIATIONS: David Geffen School of Medicine at UCLA, Department of Family Medicine
INTRODUCTION: Unhoused individuals in Skid Row experience a disproportionate burden of chronic, untreated wounds and acute illness. Without timely intervention, these conditions can progress to severe complications and death. Across Los Angeles County, over 75,000 individuals experience homelessness, with approximately 4,000–5,000 concentrated in Skid Row. Nearly 70% are unsheltered, facing significant barriers to accessing traditional healthcare. In response to these gaps, UCLA’s Student Run Homeless Clinics (SRHC), in partnership with Union Rescue Mission (URM), implemented a weekly, student-led, on-foot ‘wound-care x prayer walk’ outreach model delivering real-time wound care through relationship-centered engagement. Outreach was conducted alongside chaplain teams providing optional supportive engagement through prayer, while medical students, supervised by an attending physician, directly engaged with individuals to assess and treat wounds and acute illness on-site. The needs identified through these encounters informed the development of this quality improvement project.
METHODS: This was a mixed-methods QI project. Outreach was conducted weekly by medical students alongside community partners, including chaplain teams providing optional prayer and engagement. Clinical care, including wound assessment, treatment, and triage, was delivered in real time during encounters. Data collection included clinical characteristics (wound type, severity, acute vs. chronic), care delivered and outcomes, patient barriers to care, wound photography, and semi-structured interviews with community partners. Quantitative data were analyzed using descriptive statistics, and qualitative data will be analyzed using thematic analysis.
RESULTS: Over a 12-month period, 190 patients were evaluated and treated. Most presentations included chronic wounds and acute infections, often at advanced stages due to delayed care and limited access to hygiene resources. Patients reported limited mobility, inability to leave belongings or pets, healthcare distrust, prior negative experiences, and difficulty navigating care as key barriers to accessing services. Of those treated, 169 patients (89.0%) were successfully managed in the field, 14 patients (7.4%) received warm-hand offs to Wesley Health Center, and 7 patients (3.7%) required escalation to the emergency department.
CONCLUSIONS: This student-led, on-foot outreach model reached patients at critical moments, with 89% managed in the field. Patients frequently presented with advanced wounds and faced significant barriers to care, including mobility limitations, healthcare distrust, and concerns about belongings and pets. Through consistent, street-based engagement with community partners, patients were more willing to accept care and share concerns. Chaplain supported engagement (e.g., prayer) was well received and appeared to facilitate trust and disclosure, including previously unaddressed wounds. These findings suggest that relationship centered, community partnered approaches can improve engagement and access to care in vulnerable populations. This model offers a scalable approach to delivering low-barrier, community-based care while serving as a framework for medical student education and outreach.
Association Between GLP-1 Receptor Agonist Initiation and Changes in Cannabis Use: A Pre-Post Analysis Using the ASSIST Protocol
AUTHORS: Alexander Fish (1), Naira Setrakian (2), Marjan Javanbakht (2), and Lillian Gelberg (1,2)
AFFILIATIONS: (1) UCLA David Geffen School of Medicine; (2) UCLA Fielding School of Public Health
INTRODUCTION: Cannabis use is common in primary care populations and associated with adverse health outcomes, yet effective pharmacologic interventions are limited. Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) modulate reward pathways and may influence substance use behaviors. Real-world clinical evidence remains limited. We evaluated whether GLP-1 initiation is associated with changes in cannabis use in a primary care setting using the ASSIST protocol.
METHODS: We conducted a retrospective pre-post study of 2,229 patients with cannabis use assessed before and after GLP-1 initiation within a large healthcare system between 2022-2024. Cannabis use was measured using the ASSIST screening tool. The primary outcome was presence of cannabis use. Mixed-effects logistic regression modeled the association between post-initiation status and cannabis use, accounting for repeated measures within individuals. An adjusted model included age, sex, and race.
RESULTS: Among 2,229 patients, 1,753 (78.6%) reported no cannabis use at both timepoints, 77 (3.5%) initiated use, 123 (5.5%) discontinued use, and 276 (12.4%) reported persistent use. Cannabis use decreased from 17.9% pre-initiation to 15.8% post-initiation. Post-GLP-1 status was associated with lower odds of cannabis use in unadjusted analysis (OR 0.36, 95% CI 0.25–0.54) and adjusted analysis (aOR 0.37, 95% CI 0.25–0.54).
CONCLUSIONS: GLP-1 initiation was associated with significantly lower odds of cannabis use in this pre–post analysis. These findings support a potential role for GLP-1–based therapies as adjunctive tools in addressing substance use in primary care settings. Future studies aim to follow patients longitudinally with annual ASSIST screening to detect changes in cannabis use and associations with metabolic therapies.
Food as Medicine (FAM) in the Safety Net: Analyzing FAM Landscape and Patient-Driven Strategies to Address Food Insecurity
AUTHORS: George Heredia (1), Minal Borsada MD (2), Ann M. Hernandez MD, MPH (1)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA PRIME-LA; (2) Family Health Matters Community Health Center
INTRODUCTION: Nearly half (48%) of low-income Latino adults in California experience food insecurity, contributing to chronic disease and adverse mental health outcomes. Food as Medicine (FAM) interventions have shown promise towards embedding nutrition support within healthcare delivery and improving health outcomes. However, there is limited literature characterizing the FAM landscape within FQHC settings and the extent to which patient perspectives are incorporated into program design and implementation. This mixed-methods study evaluates the FAM landscape and engages patients to inform future FAM program development.
METHODS: This mixed-methods study combines a scoping review and qualitative data collection. A literature search of PubMed, Google Scholar, and gray literature (websites, county reports, FQHC documents, policy briefs) identifies FAM program models. Patient focus groups at an Orange County safety-net clinic explore experiences with food insecurity and perceptions of FAM. Data will be recorded and transcribed. Program characteristics will be summarized using descriptive statistics, and qualitative data will be analyzed using thematic analysis to identify key patient-derived themes.
RESULTS: Data collection is ongoing; preliminary program mapping findings and emerging qualitative themes will be presented at the time of the conference.
CONCLUSIONS: This study addresses gaps in understanding how Food as Medicine programs operate within safety-net settings and incorporate patient perspectives. By mapping regional programs and elevating patient voice, findings will inform patient-centered, sustainable FAM strategies. Results aim to guide future implementation, evaluation, and policy integration to improve food security and chronic disease outcomes among underserved populations.
Beyond Hair Loss Severity: Care-journey factors and psychosocial distress in scarring alopecia (CAPAIR)
AUTHORS: Drew Mack, BS (1); Angshuman Saha, PhD (2); Carolyn Goh, MD (1)
AFFILIATIONS: (1) David Geffen School of Medicine, University of California, Los Angeles; (2) CTSI Stats Department, University of California, Los Angeles
INTRODUCTION: Primary cicatricial alopecias cause irreversible hair loss and significant psychosocial distress. While disease severity is often assumed to drive distress, patient experience within the healthcare system may also play an important role. Prior work has emphasized stigma and illness perception, with less focus on the care journey itself. We examined whether care-journey factors contribute to hair loss–related distress beyond disease severity.
METHODS: We conducted a cross-sectional analysis of the 2022 CAPAIR survey of patients with scarring alopecia. Emotional distress outcomes included self-reported anxiety and sadness due to hair loss (binary). Hair loss severity was categorized (<25%, 25–50%, >50%). Care-journey variables included number of physicians seen (0–1 vs ≥2) and comfort discussing hair loss (comfortable vs not fully comfortable). Nested logistic regression models were used to evaluate associations, comparing severity-only models (Model 1) to models including care-journey factors (Model 2). Model fit was assessed using likelihood ratio tests.
RESULTS: Among 1,048 respondents, care-journey factors were strongly associated with distress independent of severity. Seeing ≥2 physicians was associated with higher odds of anxiety (OR 2.60, 95% CI 1.60–4.21) and sadness (OR 3.44, 95% CI 1.60–7.41). Not being fully comfortable discussing hair loss was also associated with anxiety (OR 2.07, 95% CI 1.42–3.00) and sadness (OR 2.52, 95% CI 1.16–5.46). Adding care-journey variables significantly improved model fit for anxiety (Δ deviance = 31.39, p = 1.53×10⁻⁷) and sadness (Δ = 16.49, p = 2.63×10⁻⁴). Predicted probabilities of distress were consistently higher in high-friction care contexts across all severity levels.
CONCLUSIONS: Care-journey factors, including care fragmentation and communication barriers, are strongly associated with psychosocial distress in scarring alopecia independent of disease severity. These findings suggest that improving continuity of care and patient–physician communication may meaningfully reduce distress. Interventions targeting the care experience may be as important as those addressing disease severity.
Centering Community Voices to Redesign a Black Wellness Initiative in Los Angeles
AUTHORS: Makaelah Murray (1), Makeen Yasar (2), Naomi Akhidenor (1), Fatoumata Barry (1), Akeive Burrows (1), Aarin Huffman (2), Tamia Jones (1), Dorian Kariuki (1), Martin Kyalwazi (1), Tyrah Lacey (1), Kahtrel Maynard (1), Akira McDaniels (3), Tolu Ogunrinde (1), Ezi-Nneoma Okoro (1), Elicia Osigwe (1), Danielle Shores (1), Camille Simo (1), Alexandra Thompson (1), Lauren Tucker (1)
AFFILIATIONS: (1) David Geffen School of Medicine, (2) Charles R Drew University School of Medicine, (3) UC Irvine School of Medicine
INTRODUCTION: During our first year of medical school, while serving on the SNMA E-Board, our team organized a health fair in Baldwin Village that served more than 120 community members through free health screenings and wellness activities. After seeing the unmet needs of Black patients more clearly during our clinical rotations, we sought to build something more responsive and sustainable. We partnered with Black medical students at UCLA, CDU, and UCI to form the Black Wellness Project, LA, a coalition dedicated to improving health equity for Black residents of Los Angeles County through community listening, education, and outreach.
METHODS: To launch this initiative, we secured $2,150 from Physicians for a Healthy California and $4,500 from the David Geffen School of Medicine Center of Excellence. We are using a mixed approach, including community surveys, listening sessions, and education workshops, to evaluate Black residents’ perception of health care and access in South Los Angeles. All activities take place in community spaces primarily serving Black and other historically marginalized populations in South LA.
RESULTS: To date, 44 surveys have been completed and one community listening session has been held. Preliminary findings show that most respondents were female-identifying (81.8%), Black or African American (69.8%), and between ages 27 to 64, with 47.7% reporting annual incomes above $75,000. While 90.0% reported having a primary care provider and 81.8% understood the services offered, respondents still described barriers to quality care, including limited nutritional support, lack of mental health resources, difficulty navigating services, and a need for more self-care education. At the first listening session at Jim Gilliam Park, six residents highlighted strong community assets, but emphasized that care often feels inaccessible, inconsistent, and hard to understand.
CONCLUSIONS: Our preliminary findings suggest that access to care alone does not overcome the social drivers of health. Even among many respondents who were young Black women with relatively stable incomes, gaps in supportive services remained. This supports prior work showing that Black morbidity and mortality are shaped not only by access, but also by broader social inequities within and beyond the health system. Saturday-only sampling likely missed higher-barrier groups. Overall, Black communities in Los Angeles are not monolithic, and interventions must be tailored to each community’s specific needs.
Digital Access Among Emergency Department Patients
AUTHORS: Liliana Perez, BS, MS3 (1,2); Bryant Andrade, BS (2); David Salazar, BS (2); Yesenia Perez, MS (2); Maureen McCullough, MD (2); Breena Taira, MD, MPH (2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA, (2) Department of Emergency Medicine, Olive View-UCLA Medical Center
INTRODUCTION: The rapid digitization of healthcare is transforming how patients access, navigate, and receive care, underscoring its role in promoting equity. However, many patients in safety-net emergency departments lack reliable digital access, creating barriers to scheduling, telehealth, and care coordination, and potentially worsening outcomes. Despite emerging interventions, limited quantitative data exist on the prevalence of digital access among ED patients and its relationship to healthcare use and resource awareness.
METHODS: An anonymous, cross-sectional digital survey was administered to a convenience sample of adult ED patients at Olive View-UCLA Medical Center. Trained staff verbally conducted the survey in English or Spanish, assessing digital access, healthcare engagement, and awareness of social services. Eligible patients were ≥18 years, able to consent, and not intoxicated, altered, on psychiatric hold, or in custody. Participation was voluntary (~10 minutes). Staff recorded responses and notified providers of urgent digital needs. Data were analyzed using descriptive statistics.
RESULTS: Of 100 enrolled patients, 55% were male, 72% identified as Latinx, and 16% as non-Latinx White. Spanish was the primary language for 54%, with 60% reporting limited English proficiency. Most participants had a cellphone (98%), with 95% reporting a working device and 98% having service. Home internet access was reported by 80%. Additionally, 93% had access to another electronic device, though 47% relied only on electrical outlets. A majority (68%) had a regular doctor, with 76% seen within the past 6 months. Among the 32% without regular care, 53% had not received care in the past year; 50% relied on the ED, and 22% forewent care. Awareness of the patient portal was 40%, with 53% of those using it mainly for lab results.
CONCLUSIONS: The majority of participants had a cellphone that worked and had cell service. Despite this, a large proportion did not have primary care established, nor did they utilize digital services like patient portals for their care. Digital access has increased; however, more outreach is needed to ensure that individuals are educated and empowered to manage their own care.
Silicone Disease as a Risk Factor for Inguinal Lymphadenopathy
AUTHORS: Kushagra Tewari (1), Lucas Karamanoukian (2), Manuel Mendoza, MD (3)
AFFILIATIONS: (1) David Geffen School of Medicine, UCLA; (2) Brentwood High School; (3) Department of Family Medicine, UCLA Health Toluca Lake
INTRODUCTION: In a primary care setting, the presence of inguinal lymphadenopathy may precipitate a focused clinical workup that includes both benign and malignant etiologies. Silicone disease (SD) represents a clinical pattern of autoimmune dysregulation caused by the infiltration of silicone oil within the soft tissue. Our study identifies SD as a unique etiologic cause of inguinal lymphadenopathy and phlebitis within the femoral triangle.
METHODS: A single-institution prospective cohort study was conducted on 42 consecutive patients with a history of silicone disease in the buttocks in order to assess the prevalence of non-contiguous silicone disease within the femoral triangle and inguinal region. Ultrasonographic evaluation of the femoral triangle was performed to confirm the presence of peri-lymphatic silicone disease, deep venous thrombosis, and perivascular phlebitis. We reviewed demographics (Age, Gender); prevalence of associated skin disease, inguinal lymphadenopathy, and granuloma formation in the inguinal region in those patients with a history of SD in the buttocks.
RESULTS: 42 patients with SD in the buttocks (Avg Age: 36, 100% F) were identified. The majority of patients (36 patients, 86%) had sonographic evidence of distant lymphadenopathy in the inguinal region. Post-inflammatory hyperpigmentation (30 patients, 71%) and Post-inflammatory erythema (38 patients, 90%) were present in the buttock skin; while only 2 patients demonstrated post-inflammatory erythema in the inguinal region. Twelve patients had unilateral or bilateral inguinal lymphadenopathy demonstrating non-contiguous lymphatic or hematogenous spread of silicone from the buttocks to the inguinal region. No patients demonstrated deep venous thrombosis among the 42 patients; although all patients demonstrated perivascular silicone disease.
CONCLUSIONS: Silicone disease has the potential to migrate through contiguous tissue planes, or through non-contiguous lymphatic or hematogenous channels to distant sites. In a primary care setting, the management and diagnosis of inguinal lymphadenopathy should exclude migrated silicone disease from distant sites in those patients fitting the demographic of previous silicone injections for soft tissue volumization.
Evaluating Prenatal Care Experiences and Postpartum Support Needs Among Patients Participating in Centering Pregnancy at UCLA Health
AUTHORS: Alexandra Thompson, MS3; Dae-zhané Boland, MPH; Mya Zapata, MD; Candace Gragnani, MD
AFFILIATIONS: David Geffen School of Medicine at UCLA; UCLA Fielding School of Public Health; Department of Obstetrics & Gynecology at UCLA; Division of Medicine-Pediatrics and Preventive Medicine at UCLA
INTRODUCTION: Centering Pregnancy is an evidence-based group prenatal care model associated with improved psychosocial outcomes, patient engagement, and breastfeeding initiation, yet little is known about how it is experienced within UCLA Health. Postpartum needs also remain under-addressed in routine care. This study compares Centering Pregnancy and traditional prenatal care to identify differences in support, unmet needs, and postpartum readiness and to inform development of a Centering Postpartum curriculum.
METHODS: This is a single-site qualitative study within UCLA Health. We plan to conduct semi-structured Zoom interviews with 40 postpartum patients: 20 who participated in Centering Pregnancy, including BlackCentering participants, and 20 who received traditional prenatal care. Eligible participants are age 18 or older, English-speaking, delivered at UCLA on or after April 1, 2025, and had at least 3 prenatal visits at UCLA. Interview domains include prenatal care experience, cultural relevance, support, stress, postpartum transition, and accessibility. Data will undergo thematic analysis in Dedoose.
RESULTS: Recruitment and data collection are underway. Planned enrollment includes 40 postpartum participants across Centering Pregnancy and usual care groups. Preliminary outcomes of interest include perceived support, preparedness for postpartum recovery, access to resources, and program accessibility. Planned analysis will compare emergent themes across care models and identify cross-cutting domains relevant to curriculum development, including mental health, lactation support, trust in care teams, and structural barriers to postpartum follow-up. Results will be presented if available at the time of the meeting.
CONCLUSIONS: This study will provide early qualitative evidence on how group versus traditional prenatal care is experienced within UCLA Health. Findings are expected to identify actionable gaps in postpartum support and inform a patient-centered Centering Postpartum curriculum. This work may also highlight opportunities to improve continuity, equity, and emotional support in perinatal care.
Assessing and Addressing Barriers to Cancer Screening Among Housing-Insecure Women in Downtown Los Angeles
AUTHORS: Margo Williams (1), Jessica Menjivar Cruz (1), Mary Marfisee, MD, MPH (2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA; (2) Department of Family Medicine at UCLA
INTRODUCTION: Compared to the national average, unhoused women demonstrate significantly lower rates of cervical and breast cancer screenings and experience higher rates of late-stage cancer diagnoses. These inequities have complex underlying causes which go beyond just cost or availability of services, and thus require multifaceted solutions tailored to local conditions. This project is a pilot program facilitating on-site screening mammography and Pap smears for housing-insecure women residing at Union Rescue Mission, a shelter on Skid Row, while utilizing qualitative research to assess and refine clinical and educational efforts.
METHODS: The data collection and analysis portion of this project utilizes qualitative methods, including the use of written surveys and semi-structured focus group discussions. Notes will be taken by facilitators during group discussion, and themes will be coded after comparison of discussion takeaways for analysis. The co-authors have also documented the decision-making and logistical process for establishing implementation of clinical services as well as educational programming.
RESULTS: Since December 2025, this initiative has hosted educational town halls on breast and cervical cancer screening, each including distribution of hygiene kits, as well as an on-site mammography event in partnership with City of Hope. Data collection is ongoing. We have encountered prominent themes of negative past experiences with healthcare providers and screenings, themselves, lack of knowledge on the guidelines for and utility of cancer screenings, and prohibitive time and financial burdens as significant barriers faced by this population. Surveys returned on educational events (total of 27 surveys returned, respondent ages 18-72) have shown the greatest interest in education surrounding nutrition, mammograms, and Pap smears, and the least interest in family planning and menopause.
CONCLUSIONS: Efforts to date support the efficacy of on-site educational and clinical efforts in ameliorating some barriers to cancer screenings among women at Union Rescue Mission. Alongside ongoing efforts to provide cervical cancer screenings, plans for expanded mammography events in partnership with other organizations in Skid Row are underway, illustrating the ways such events can assist in coalition-building. By using research to refine our educational and clinical interventions, our hope is to practice scholarship that works towards stronger community partnership alongside greater access to care.
ACE-Related ICD-10 Documentation among Insured Adolescents: National Comparison with Survey-Based Estimates
AUTHORS: Lisa Barkley, MD; Ehsan Yaghmaei, PhD; and Mohsen Bazargan, PhD
AFFILIATIONS: Department of Family Medicine, Charles R. Drew University of Medicine and Science
INTRODUCTION: Adverse childhood experiences (ACEs) are highly prevalent among U.S. adolescents based on national surveys, yet their documentation in administrative claims remains unclear. Recent data from the Youth Risk Behavior Survey and National Survey of Children’s Health show substantial exposure to ACEs, including abuse and household dysfunction. This study aims to quantify the frequency and patterns of ACE-related ICD-10 documentation in claims data and compare these findings with national survey estimates.
METHODS: We conducted a descriptive analysis of administrative claims data from 2019–2024 for insured adolescents aged 12–18 years with at least one healthcare encounter. ACE-related documentation was identified using ICD-10 codes for abuse history, abuse-related mental health encounters, clinical examinations following suspected abuse, family disruption, and household substance abuse. Outcomes were summarized as percentages and rates per 1,000 adolescents across national, state-year, and insurance-type levels using descriptive statistics.
RESULTS: ACE-related ICD-10 documentation was consistently rare across all years and levels. Fewer than 0.1% of adolescents had any documented ACE-related code annually. Family disruption was the most frequently recorded condition (0.95 per 1,000), followed by abuse-related mental health encounters (0.40) and abuse history (0.28). Household substance abuse (0.14) and abuse-related examinations (0.10) were least common. Substantial variation existed across states, with many reporting zero cases. Claims-based estimates were markedly lower than national survey findings.
CONCLUSIONS: ACE-related ICD-10 documentation in claims data is exceedingly low compared with national survey estimates. These findings suggest that claims data capture only a small fraction of underlying adversity exposure and likely reflect clinical recognition and coding practices rather than true prevalence. This underdocumentation highlights potential gaps in screening, assessment, and coding of ACEs in routine clinical care.
Medicaid Policy Changes and Immigration Enforcement: Impacts on Healthcare Access, Delivery and Patient Experience in Los Angeles County Safety-Net Clinics
AUTHORS: *Lilia Diaz (1), *George Heredia (1), *Diana Jimenez-Briseno (1), *Dorian Kariuki (1), *Iman Kazah (1), *Makaelah Murray (1), Don Garcia, MD (3) Arthur Ohannessian, MD (4), Parastou Farhadian MD (5), Cesar Barba, MD (6), Gerardo Moreno, MD, MS, MSHS, and Dr. Ann Marie Hernandez MD, MPH (1,2)
AFFILIATIONS: (1) David Geffen School of Medicine at UCLA; (2) Department of Family Medicine at UCLA; (3) Clínica Monseñor Oscar A. Romero, Los Angeles, CA; (4) Mid Valley Health Center, LAC DHS, Los Angeles, CA; (5) Mission Community Hospital, Panorama City, CA ; (6) Venice Family Clinic, Venice, CA. *These authors contributed equally to this work.
INTRODUCTION: Recent federal Medicaid policy changes under the H.R.1 bill may reduce safety-net financing and disproportionately affect low-income, uninsured, and undocumented populations. Prior Medicaid funding reductions have been linked to decreased access, reduced services, and 1strained clinic capacity. Simultaneously, heightened immigration enforcement may further deter healthcare utilization. This three-part mixed-methods study examines patient and stakeholder understanding and experience while assessing early shifts in care access and outcomes at Los Angeles safety-net clinics.
METHODS: The current study focuses on patients and ancillary staff (community health workers) within a coordinated three-part mixed-methods design including patients, ancillary staff, clinicians, and administrative leadership across 4 Los Angeles County safety-net clinics, in parallel collaborating studies. The current study employs semi-structured interviews with patients and ancillary staff conducted at 2 community health centers in Los Angeles to explore their understanding of the anticipated H.R.1 policy changes and the impact of immigration enforcement on healthcare access, delivery and experience. This qualitative data will be analyzed using thematic analysis.
RESULTS: Data collection is ongoing. Initial review of the first six patient interviews suggests emerging themes related to immigration-related fear and psychological distress, financial strain and structural barriers to care, disruptions in healthcare engagement, clinics as trusted spaces for safety and information and uncertainty about H.R.1-related insurance changes. These observations are exploratory. Qualitative analysis is ongoing.
CONCLUSIONS: As safety-net clinics navigate pressures from Medicaid restructuring and immigration enforcement, understanding their intersecting effects on vulnerable populations is urgent. This patient and ancillary staff-focused arm of a coordinated three-part study complements parallel clinician and administrative leadership qualitative analyses. The approach captures system-level trends and lived experiences often absent from policy discussions. Findings aim to inform clinic-level adaptations and advocate for policy safeguards protecting equitable access for LA based underserved communities and beyond.
Cabrillo Room - Case Reports
Isolated Group A Streptococcal Psoas Abscess in an Immunocompetent Young Woman: A Rare Post-Gynecologic Complication
AUTHORS: Zuhair Chaudhry OMS III, Saher Zaidi OMS III, Rachel Battersby OMS III, Jessica Avila MD, Cathy Vu DO, Ebenezer Dadzie MD, Jose Urbina MD
AFFILIATIONS: Western University of Health Sciences, Kern Medical Center, Clinica Sierra Vista - Rio Bravo Family Medicine Residency Program
INTRODUCTION: Psoas abscess is a rare but serious infection most commonly caused by Staphylococcus aureus or enteric organisms. Streptococcus pyogenes is an exceptionally rare etiology, reported only in isolated cases. Invasive Group A Streptococcus (GAS) infections may follow gynecologic procedures and can occur in otherwise healthy individuals. This case highlights an atypical presentation of GAS bacteremia with psoas myositis and developing abscess in an immunocompetent patient.
METHODS: A previously healthy 21-year-old woman presented with 10 days of worsening bilateral leg pain, fever, and inability to walk, beginning 2 weeks after a medication-induced abortion. On admission, she was febrile, tachycardic, and had marked leukocytosis (32,000/μL) with elevated inflammatory markers. Because of severe pain and limited mobility, neurologic pathology was initially suspected. Lumbar puncture showed CSF pleocytosis, and empiric meningitis treatment was started. Blood cultures later grew Streptococcus pyogenes, confirming bacteremia, and antibiotics were narrowed. Neurology determined meningitis was unlikely, with findings more consistent with a parameningeal inflammatory response. CT abdomen/pelvis showed inflammation of the psoas and iliacus muscles, with repeat imaging revealing a small developing psoas abscess not suitable for drainage. No other infectious source was identified. She improved with targeted IV antibiotics and supportive care, regained independent ambulation, and was discharged on oral antibiotics with outpatient follow-up.
DISCUSSION: GAS-associated psoas abscess is rare, especially in immunocompetent patients without classic risk factors. In this case, recent medication-induced abortion likely provided the portal of entry through mucosal disruption and hematogenous spread. Diagnosis was challenging because the presentation mimicked meningitis, including sterile CSF pleocytosis, likely reflecting a parameningeal inflammatory response rather than CNS infection. Small abscesses may be managed successfully with antibiotics alone when the patient is clinically stable and drainage is not feasible. Clinicians should maintain suspicion for deep retroperitoneal infection in post-gynecologic patients with severe pain and systemic illness, even without localizing gynecologic symptoms. Early imaging and targeted therapy are key.
Refractory Fetal Supraventricular Tachycardia with Hydrops Fetalis and Mirror Syndrome
AUTHORS: Ivy Hsu, DO, Jesse Cheung, MD, Surya Lakhanpal, MD
AFFILIATIONS: Pomona Valley Hospital Medical Center FMRP
INTRODUCTION: Fetal supraventricular tachycardia (SVT) is a rare but potentially life-threatening arrhythmia that can lead to hydrops fetalis and significant perinatal morbidity and mortality. Early recognition and management are critical but can be challenging, particularly in refractory cases.
METHODS: A 26-year-old primigravida at 29 weeks of gestation, late to prenatal care, presented with fetal tachycardia up to 300 bpm. Her pregnancy was complicated by chronic hypertension, diet-controlled gestational diabetes, and alpha thalassemia carrier status. Ultrasound demonstrated severe hydrops fetalis with diffuse anasarca and large-volume ascites. Persistent fetal tachycardia (280–300 bpm), concerning for SVT or atrial flutter, was noted. Transplacental therapy with digoxin and flecainide failed to achieve sustained rhythm control. The course was further complicated by maternal transaminitis and anemia concerning for mirror syndrome, prompting cesarean delivery at 29 weeks and 5 days. The newborn was delivered breech with severe hydrops and respiratory distress requiring immediate intubation, high-frequency ventilation, and paracentesis. SVT remained refractory to adenosine and multiple synchronized cardioversions, necessitating vasopressor support and transfer for advanced cardiac care.
DISCUSSION: This case illustrates the rapid progression and high morbidity associated with refractory fetal SVT, particularly once hydrops fetalis has developed. While transplacental antiarrhythmic therapy is first-line management, its effectiveness may be limited in advanced disease with significant fluid overload. Additionally, this case highlights the development of maternal complications, including suspected mirror syndrome, necessitating careful monitoring for maternal end-organ dysfunction. Multidisciplinary coordination is essential, and early delivery should be considered when there is evidence of worsening maternal status or nonresponse to therapy.
Postural Orthostatic Tachycardia Syndrome in an Adolescent Male: A Case Report
AUTHORS: Kyung Kim, MD (1); Laura Hernandez, MD (1); Carmen van den Heever, MSIII (2); Yasmeen Rabiei, MSIII (2); Victoria Huynh, MSIII (2); Davit Martirosyan, MSIII (2); Thiagarajan Nandhagopal, MD (3)
AFFILIATIONS: (1) Rio Bravo Family Medicine Residency; (2) Western University of Health Sciences; (3) Kern Medical
INTRODUCTION: Postural orthostatic tachycardia syndrome (POTS) is a disorder of orthostatic intolerance most commonly seen in adolescent females. Neuropathic subtype, the most common form of POTS, may present with lower extremity pain and sensory symptoms, broadening the differential to include structural, neurologic and cardiac causes. We present a case of suspected neuropathic POTS in an adolescent Hispanic male whose complex symptomatology initially raised concern for alternative diagnoses before autonomic dysfunction was considered.
METHODS: A 14-year-old male with no significant past medical history presented on 8/12/2025 with intermittent right-sided chest pain radiating to the back, dyspnea, and lightheadedness. Electrocardiogram was unremarkable, and he was discharged. He subsequently developed progressive bilateral lower extremity pain, subjective weakness, numbness, perianal sensory changes, and worsening gait instability. On 8/16, he fell while attempting to stand from the toilet, striking his head without loss of consciousness. He returned on 8/18 with persistent chest pain, severe bilateral leg pain with sensory changes, impaired balance, and orthostatic symptoms. Examination demonstrated inconsistent lower extremity sensation and strength with intact reflexes and no true focal deficits, though gait instability was consistently observed. Physical therapy noted decreased step length and anterior lean requiring a front-wheel walker. Extensive workup, including MRI of the brain and spine, CTA chest, echocardiography, and laboratory studies, was unremarkable. Orthostatic vitals revealed tachycardia, supporting POTS.
DISCUSSION: This case highlights the diagnostic challenge of POTS presenting with neurologic symptoms. Bilateral lower extremity complaints and perianal numbness raised concern for spinal cord pathology, but variable exam findings, preserved reflexes, and normal imaging argued against structural disease. POTS is increasingly recognized as a multisystem condition with fatigue, pain, and cognitive symptoms beyond orthostatic intolerance, and adolescent presentations may be atypical or overlap with functional features. Early consideration of POTS in patients with inconsistent neurologic findings and negative workup may reduce unnecessary testing. Orthostatic vitals remain a simple, critical diagnostic tool.
Catalina Room - Abstracts
Implementation of a 3-day deadline on take-home colorectal cancer screening test return rates
AUTHORS: Alison Butler, MD PhD, John Cheng, MD, Monica Le, MD MPH
AFFILIATIONS: Department of Family Medicine, Harbor-UCLA Medical Center
INTRODUCTION: Colorectal cancer (CRC) is both the third most diagnosed cancer and the third highest cause of cancer death. Unfortunately, CRC screening rates at our clinic with our healthcare system’s first line test, the fecal immunochemical test (FIT), have been persistently below the system-wide target screening rate. Prior studies have shown that setting a specific return time increases the rate of screening test completion. We proposed that implementing a 3-day return “deadline” when distributing FIT kits in our clinic would lead to improved FIT completion rates and faster return times compared to standard test distribution.
METHODS: Prior to November 2025, patients who were eligible for CRC screening had received the normal FIT envelope and instructions for completing the test. We created a bilingual (English + Spanish) FIT insert card to include with the FIT envelope patients receive in the clinic. The card featured a designated space for nursing staff to write in a “due date” that would be 3 days from the day the kit was administered. In addition, nursing staff and providers verbally encouraged a 3-day return window when giving instructions for completing the test at home. Starting November 1, 2025, all eligible patients received the FIT insert with their test. A time series analysis model was used to compare immediate changes and gradual trends in FIT return rates after implementation of the 3-day deadline.
RESULTS: The intervention is still ongoing. However, since implementation of the FIT return deadline in November 2025, CRC screening rates in our clinic have steadily improved. As of January 2026, our clinic screening rate has exceeded the county-wide target of 58%. Moreover, the average time to return the FIT for our clinic patients has steadily decreased, specifically from 19.8 days in October 2025 (the month before the intervention began) to 9.4 days in March 2026.
CONCLUSIONS: This project demonstrates how a simple, cost-effective intervention can improve CRC screening completion in a clinic serving socioeconomically disadvantaged patients. If a written and verbal deadline can successfully increase FIT return rates such that they exceed the county-wide target, then the application of this quality improvement intervention extends to other quality improvement metrics that are contingent on patient compliance with instructions in a timely manner.
Most Common Reasons for No-Shows in the Outpatient Clinic Setting
AUTHORS: Haik Chatalyan, DO, Katherine Adler, MD, and Nadia Chavez Mora, MD
AFFILIATIONS: Dignity Health - Northridge Medical Center
INTRODUCTION: Missed appointments (“no-shows”) in outpatient clinics represent a persistent challenge for healthcare systems. No-shows negatively affect clinic efficiency, provider productivity, continuity of care, patient outcomes, and healthcare costs. Understanding patient-reported reasons for missed appointments is essential to designing targeted interventions that improve attendance, optimize resource utilization, and enhance patient-centered care.
METHODS: This is a cross-sectional, minimal risk, prospective study using structured telephone interviews of adult patients who recently no-showed for an outpatient clinic appointment. Fifty eligible patients (recent no-shows) contacted by phone, verbal consent obtained, and structured interview conducted (~5 minutes). Predefined response options and free-text allowed. Participation occurs in one phone call; no follow-up. Statistical method used to analyze the data is a Pareto chart.
RESULTS: A total of fifty patients were interviewed for reasons for no-shows to identify most common contributing factors; and results were analyzed via a Pareto chart. The leading reason for missed appointments was forgetting the appointment or not receiving a reminder. Work-related conflicts were the second most common factor, followed by patients reporting that the appointment was no longer needed and illness-related reasons. Additional contributors included insurance-related issues, transportation barriers, and conflicting appointments, while scheduling conflicts and family emergencies were less frequently reported.
CONCLUSIONS: Outpatient no-shows are largely driven by a small number of predominant and potentially modifiable factors. Interventions targeting improved reminder systems, increased scheduling flexibility, and enhanced patient communication regarding appointment necessity may substantially reduce missed appointments. Addressing these high-yield contributors could improve clinic efficiency, patient access to care, and overall healthcare delivery outcomes.
Increasing Family Medicine Resident's Confidence in Musculoskeletal Point-of-Care Ultrasound
AUTHORS: Bret Chavarria MD, Michael Li PhD MPH, and Jack Chen MD
AFFILIATIONS: Department of Family Medicine at UCLA
INTRODUCTION: Point of care ultrasound (POCUS) is an emerging clinical tool with vast potential, as seen with its growing use in health care. However, it does require specialized training. Currently, there is no standardized Musculoskeletal (MSK) POCUS curriculum for Family Medicine (FM) Residencies. As much as 40% of visits are for MSK complaints. Thus, utilization of MSK POCUS can prove to be an effective tool for diagnosis and treatment. The goal of this study is to evaluate the effectiveness of one-on-one teaching sessions for MSK POCUS training.
METHODS: UCLA FM residents, 12 per class for 36 total, were recruited for this study. Interns participated during a dedicated POCUS course, while PGY 2/3’s had optional participation. Before the teaching sessions, residents completed a pre-survey looking at confidence in six areas: knobology, transducer selection, patient positioning, structure identification in short and long axis, image optimization and dynamic evaluation. Each area was based on 5-point confidence level, starting at ‘not at all’ to ‘extremely’ confident. Participants then underwent two one-hour one-on-one sessions with an MSK POCUS trained attending. Participants then completed the same survey after the second session. Surveys were paired via participant, and analysis was run via paired T-test.
RESULTS: Data was analyzed utilizing Strata MP Version 19. Each variable was analyzed for improvement in confidence from pre to post survey per individual. A total of 7 participants completed the pre and post survey questionnaire. Mean difference, 95% CI and P value for were calculated for all six variables. Knobology mean difference 1.29 points (CI [0.67,1.90], p<0.001), transducer selection mean difference 1.57 points (CI [1.13, 2.01], p<0.001), patient position mean difference 1.71 points (CI [1.29,2.13], p<0.001), structure identification in short and long axis mean difference 1.14 points (CI [0.76, 1.53], p<0.001), image optimization mean difference 1.14 points (CI [0.64, 1.64], p<0.001), and dynamic evaluation mean difference 1.29 points (CI [1.02, 1.56], p<0.001).
CONCLUSIONS: Two one-hour one-on-one sessions with MSK POCUS trained attending improved FM residents' confidence in MSK POCUS. These findings indicate the proposed curriculum and method to be an efficient and effective way to train family medicine residents in MSK POCUS. The limitations of this study include small sample size, attending's skill level, and the use of residents' self-reported confidence as a proxy for competency. Future research should assess residents' mastery via independent scanning and collecting a set number of "scans" per body part.
Health Costs of Urban Oil and Gas Drilling in Los Angeles
AUTHORS: Amanda d’Almeida MD, MPH (1), Emma Silber (2)
AFFILIATIONS: (1) UCLA Department of Family Medicine; (2) PSR-LA; STAND-LA
INTRODUCTION: Oil and gas drilling in Los Angeles dates back to the 1890s; the city currently has ~5,000 active, idle, or abandoned wells. One-third of LA County residents live within one mile of a well, with disproportionate impacts, 92% of nearby residents are people of color (2) and poverty rates are 40% higher in high-density well areas than the rest of the county (3). Proximity to oil and gas operations has been linked to premature death, preterm birth, and respiratory disease.Through the advocacy of STAND-LA, an environmental justice coalition, the question has arisen: what is the economic cost of health impacts from upstream oil and gas operations?
METHODS: We conducted a secondary data analysis to inform a Health Impact Assessment using validated data from Vohra et al., 2025, stratified by state, pollutant, health outcome, and lifecycle stage. Health outcomes included premature mortality, preterm birth, asthma, and cancer incidence. Los Angeles County-specific data were obtained directly from the authors. We applied the EPA's Value of a Statistical Life to estimate economic burden and reviewed three LA City Council-commissioned amortization studies, Baker & O'Brien (B&O), Alvarez & Marsal (A&M), and CJM Petroleum Consulting Inc. (CJM), to model cost savings from an accelerated phase-out. Surface pollutant data from Vohra et al. will be applied to BenMAP, if applicable, to further estimate economic burden across additional health outcomes.
RESULTS: In 2017, upstream oil and gas operations caused an estimated 158 premature deaths in California (123 PM₂.₅, 27 NO₂, 8 O₃), valued at $1.58 billion using the EPA's Value of a Statistical Life. In Los Angeles County, PM₂.₅ alone caused 60 premature adult deaths, representing ~$600 million in economic burden. A 20-year phase-out projects to $12 billion in LA County and $31.6 billion statewide in premature death costs. All three amortization studies support a 2028 phase-out: B&O found a median amortization of two years; A&M found 686 wells amortized by 2027; CJM found 93–95% amortized by 2028. A 2028 phase-out would save LA County ~$10.2 billion and California ~$26.86 billion. Asian, Black, Hispanic, and Native American populations bear the greatest exposure burdens across all lifecycle stages.
CONCLUSIONS: Urban oil and gas drilling in Los Angeles imposes substantial economic and health costs, with premature deaths alone costing LA County ~$600 million annually. These burdens fall disproportionately on communities of color and low-income residents. We recognize the human toll extends beyond any economic figure; nevertheless, quantifying these costs provides powerful evidence for policy action. Amortization data support a 2028 phase-out, potentially saving LA County $10.2 billion and California $26.86 billion in economic burden.
Optimizing the Adolescent Transition: A Population-Based Approach to PECARN Adherence in Trauma Care
AUTHORS: Ngoc Duong, DO, Alex Kertzner, MD, PhD, Anisha Patel, DO, Nensey Cyrus, MD
AFFILIATIONS: Dignity Health Family Medicine Residency Northridge
INTRODUCTION: Patients aged 12–17 are at the intersection between pediatric and adult medicine. The PECARN Pediatric Head Injury Algorithm is validated to exclude CT imaging in low-risk patients under 18, minimizing unnecessary radiation exposure. NHMC uses an age-based cutoff to determine pediatric vs. adult trauma management. Patients under 14 managed by Pediatric Trauma Surgeons (TS). Patients 14 and older managed by Adult TS. This study assesses whether transitioning to adult management at age 14 is associated with differences in appropriate CT ordering in adolescents.
METHODS: This is a retrospective study using TEMIS at NHMC (January 2009–December 2022). Patients will be stratified into ages 12–13 (pediatric oversight) and 14–17 (adult oversight). Clinical variables include GCS, mechanism of injury, and clinical presentation. The frequency of nonindicated CT scans according to PECARN criteria will be compared between groups.
RESULTS: Recognizing the unique needs of the 12–17 age group may be important for ensuring that older adolescents do not lose access to pediatric safety standards as they transition toward adult-oriented care. Integrating PECARN principles into acute trauma, urgent care, and emergency settings may help ensure adolescents receive age-appropriate, evidence-based care while minimizing unnecessary radiation exposure.
CONCLUSIONS: The 12–17 age group warrants recognition as a distinct clinical demographic. Integrating Got Transition principles into acute trauma and emergency settings can help ensure adolescents receive age-appropriate, evidence-based care — minimizing unnecessary radiation and supporting better outcomes across the transition period.
Launching Park Rx Los Angeles County: Provider-Identified Facilitators and Barriers in a Safety Net Referral Model
AUTHORS: Tony Kuo, MD, MSHS (1)(2)(3), Eloisa Gonzalez, MD, MPH (3), Lisa Arangua, MPP (3), Rebecca Reeves, PT, MPT (3), Samantha Bonilla-Rivas, MPH (3)
AFFILIATIONS: (1) UCLA Fielding School of Public Health; (2) Department of Family Medicine, UCLA David Geffen School of Medicine; (3) Los Angeles County Department of Public Health
INTRODUCTION: Primary care providers are essential to implementing community-clinical physical activity programs, yet resource awareness and workflow barriers may limit adoption in safety net settings. Park Rx Los Angeles County (Park Rx LAC) engages providers to refer adult patients to free park-based programs. Leveraging existing provider information dissemination pathways (e.g., standing clinic meetings, physician huddles) can be key to this process. Understanding provider-identified facilitators and barriers, including clinic workflow, and program accessibility and awareness, is critical for designing scalable referral models.
METHODS: The Los Angeles County Department of Public Health recruited primary care providers from two safety net hospitals. Multiple Plan-Do-Study-Act (PDSA) cycles were conducted to elicit feedback on implementation, generating change ideas. Data sources included structured feedback, workflow discussions, and iterative refinements. Provider-reported facilitators and barriers related to knowledge of this new resource, eligibility, referral processes, program quality, and clinic integration were coded using thematic analysis and synthesized into key lessons.
RESULTS: Providers identified key facilitators and barriers. Clarifying eligibility (adults, ambulatory, medically stable, interested) improved referral confidence, but providers felt all patients could benefit from being referred. Providers also sought reassurance that programming was high-quality, culturally sensitive, and accessible. A HIPAA-compliant referral platform enabled tracking but was burdensome despite provider training; providers preferred a one-click referral and direct patient follow-up. Provider champions co-designed low-burden workflows. Waiting room patient promotion video to reduce provider burden was limited at some sites by nonfunctional screens requiring IT repair. Program expansion occurred with growing provider interest as awareness of this new resource organically spread.
CONCLUSIONS: Provider adoption depends on spreading awareness of the referral resource, minimizing workflow burden and building trust in program quality and accessibility. Simple referral processes, clear eligibility, and provider-informed workflows are key facilitators. Addressing infrastructure barriers and reducing referral complexity are critical to sustaining community-clinical physical activity programs in safety net systems.
Are We Asking the Right Questions? AUDIT-C Limitations in Longitudinal Care
AUTHORS: Alexandra Hospodar MD (1), Bianca Robertson MD (1), Ana S Ortiz (2), Katherine G Meneses (2), Susan Kang (2), Jasleen Singh MD (2,3), Julio Meza MD (1), Sammy Saab MD (2,3), Akshay Shetty MD (2,3)
AFFILIATIONS: (1) Department of Family Medicine at UCLA; (2) Department of Surgery at UCLA; (3) Department of Medicine at UCLA
INTRODUCTION: Approximately 20% of primary care patients drink at unhealthy levels, and alcohol-associated liver disease is the leading cause for liver transplantation in the U.S (2). The AUDIT-C (a validated screening tool that identifies harmful drinking) is currently being used to monitor alcohol use after liver transplant, although recipients from our liver transplant clinic report dissatisfaction with the AUDIT-C. Developing a more accurate screening tool for this population would be beneficial to monitor for continued alcohol use after a period of sobriety, and has the potential to be utilized in various clinical settings.
METHODS: This prospective, single-center, cross-sectional survey study enrolled liver transplant recipients with a diagnosis of alcohol-related liver disease and alcohol use disorder. Participants completed the standard AUDIT-C questionnaire (assessing alcohol use in the past year), the novel AUDIT-LT questionnaire (assessing alcohol use since transplant), and a 10-item patient satisfaction survey comparing both tools using a 5-point Likert scale. Demographic and clinical data including transplant characteristics, laboratory values such as Phosphatidylethanol (PEth) biomarker levels, and alcohol use history were collected from medical records. The primary outcomes were patient satisfaction ratings and qualitative feedback comparing the two screening tools. (1)
RESULTS: Forty patients were included (mean age 46.8 years; 21 male, 19 female); 14 were <12 months post-transplant. In this subgroup, 7/14 had identical scores (0 on both tools), while 7/14 screened positive on AUDIT-C but negative on AUDIT-LT, suggesting reduction is false-positive rates. All patients <12 months had PEth <10. Seven patients had positive PEth, all <12 months post-transplant; all screened positive on both tools with no observed difference in detection.
Overall, 12 patients reported higher satisfaction with AUDIT-LT compared to AUDIT-C. Eleven preferred AUDIT-LT for assessing current alcohol use, and 9 reported it more accurately reflected recent use. Thirty-one found AUDIT-LT easy to interpret. A minority reported difficulty (n=9) or emotional distress (n=7), similar to
CONCLUSIONS: Our results show a discrepancy between AUDIT-C and AUDIT-LT scores suggesting that AUDIT-C has limitations in reporting alcohol use in this population. AUDIT-LT scored almost 20% higher on patient satisfaction surveys when compared to AUDIT-C. Patient satisfaction was most evident among patients 12 months from transplant. Future studies can focus on expansion and adaptation of this screening tool to use in different clinical settings, such as monitoring alcohol use after a diagnosis of Alcohol Use Disorder has been made, and the journey to sobriety has begun.
Increasing Self-Efficacy in Cognitive Behavioral Therapy Skills in Family Medicine Residents
AUTHORS: Rebecca Li, MD, Jesse Kao, MD, MFT
AFFILIATIONS: Department of Family Medicine at UCLA
INTRODUCTION: Cognitive behavioral therapy (CBT) is an evidence-based, first-line treatment for common primary care behavioral health concerns including anxiety, depression, insomnia and substance use disorders. Up to 75% of primary care visits address at least one behavioral or mental health concern. Despite the prevalence of these concerns, primary care residents report deficits in their training and report interest in learning more about behavioral health. Equipping family medicine residents with practical tools is key to delivering evidence-based behavioral health care in the primary care setting.
METHODS: A traditional pre and post-survey design was used to evaluate the impact of a four-week CBT educational intervention among family medicine residents (pre n=5, post n=5). A pre-survey was given at the beginning of the rotation and the same questions were given at the end of the rotation. The intervention included one-on-one supervised patient encounters with an attending physician with experience in CBT, didactic lectures, handouts, and review of book chapters on brief cognitive behavioral interventions. Topics reviewed included CBT for depression, anxiety, ADHD, and insomnia. Changes in resident confidence in applying CBT skills before and after educational intervention were analyzed using a paired t-test.
RESULTS: A preliminary analysis revealed that participation in the four-week behavioral health curriculum was associated with several statistically significant outcomes. Residents demonstrated increased comfort in identifying maladaptive cycles (p=0.037) and applying CBT techniques in clinical practice (p=0.021). Residents also reported adequate time to implement these interventions in the clinical setting (p=0.035). Measures related to teaching diaphragmatic breathing (p=0.061) and performing CBT for insomnia (p=0.080) were not significant but trended toward greater comfort in each category. After completion, residents expressed being either very interested or extremely interested in learning more about behavioral health and CBT.
CONCLUSIONS: Preliminary results support the value of a behavioral health curriculum in family medicine training. Although some residents had prior exposure to behavioral health and CBT, the four-week rotation improved residents’ confidence in several CBT skills and highlighted areas for improvement. Residents reported having enough time to use these techniques and reported that the lessons learned can be incorporated into routine patient encounters. There is growing interest among family medicine residents and a dedicated curriculum can strengthen CBT skills and improve access to behavioral health care.
Text Me, Alexis! Findings from a terminated comparative-effectiveness trial of gender-affirming theory-based text messaging and peer health navigation to improve HIV care engagement and health outcomes
AUTHORS: Michael Li, PhD, MPH (1); Sean Murphy, PhD (2); Cathy Reback, PhD (3)
AFFILIATIONS: (1) University of California, Los Angeles; (2) Weill Cornell Medicine; (3) Friends Research Institute
INTRODUCTION: Transgender women living with HIV face substantial structural barriers to healthcare utilization, retention in care, and viral suppression. Gender-affirming, evidence-based interventions are therefore essential to efforts aimed at Ending the HIV Epidemic among this population.
METHODS: Text Me, Alexis! is a comparative effectiveness trial evaluating three conditions: (1) a gender-affirming peer health navigation intervention (the Alexis Project), (2) a gender-affirming theory-based text messaging intervention, and (3) a combined intervention. A total of 71 transgender women living with HIV were block randomized by race and age in a 1:1:1 ratio. HIV viral load was obtained from participants' medical providers. Participants self-reported their most recent HIV care visit and adherence to antiretroviral therapy (ART).
RESULTS: We report rates of linkage to HIV care and viral suppression across baseline, 3-month, and 6-month follow-up visits, comparing outcomes across all three conditions. We also examine self-reported ART adherence, substance use, and sexual risk behaviors over time.
CONCLUSIONS: Findings from this trial provide descriptive evidence on outcomes across the three intervention conditions, with implications for identifying whether peer navigation, text messaging, or their combination is most effective for supporting transgender women along the HIV care continuum. Termination of this grant resulted in incomplete data, limiting statistical power and our ability to make important inferences that can inform care in this high priority community for Ending the HIV Epidemic.
Catalina Room - Case Reports
Management of Treatment-Refractory MOGAD Exacerbation: A Case Report
AUTHORS: Cesar Aguilar Martinez, MD (1), Nadia Esquivel, MD (1), Lianna Navar, MD (1), Alex H Kim, MD (2)
AFFILIATIONS: (1) Department of Family Medicine at RUHS/UCR; (2) Department of Radiology at RUHS
INTRODUCTION: Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) is an autoimmune inflammatory demyelinating disorder of the CNS. Although MOGAD generally has a favorable prognosis, a subset of patients experience relapsing exacerbations with cumulative neurological disability and require long-term immunosuppressive therapy. First-line treatment for exacerbations is a 3-5 day course of high-dose IV steroids. For steroid-resistant cases, PLEX and IVIG are viable options. Emerging evidence supports the use of tocilizumab, for acute and maintenance therapy in treatment-refractory cases.
METHODS: A 25-year-old nonverbal, deaf female with a PMH of MOGAD encephalitis and bilateral optic neuritis presented to RUHS ED with progressive encephalopathy following multiple MOGAD flares. MRI brain obtained demonstrated extensive expansile bilateral hemispheric edema with 5mm midline shift and uncal herniation, significantly worse compared to prior MRI. Given concerns for MOGAD exacerbation, she was initiated on high-dose IV steroids and subsequently IVIG, however her clinical course deteriorated, requiring MICU transfer for close neurological monitoring and management of cerebral edema. Given her failure to respond adequately to steroids and IVIG, tocilizumab was administered on hospital day nine, with a second dose given three days later. Within 24 hours of the first tocilizumab dose, repeat MRI was obtained and there was near-complete resolution of abnormal enhancement and improvement in mass effect. She was subsequently downgraded from the MICU, transitioned to oral steroids, and discharged on hospital day 18 with ongoing improvement in mentation noted at time of discharge.
DISCUSSION: This case illustrates the diagnostic and treatment challenges of relapsing, refractory MOGAD. Our patient experienced multiple exacerbations within a short period, and this admission was her most severe. Despite treatment with high-dose IV steroids and IVIG, she continued to clinically deteriorate, underscoring the limitations of standard therapy in refractory cases. The rapid clinical and radiographic improvement observed shortly after tocilizumab administration highlights the potential role of IL-6 signaling in MOGAD pathophysiology. IL-6 blockade may attenuate the neuroinflammatory cascade driving cerebral edema in severe MOGAD cases. While tocilizumab use in MOGAD remains largely anecdotal, this case adds to the growing body of evidence supporting its use in refractory disease.
Bladder and Biliary Blues: A Case of Ketamine-Induced Cystitis and Cholangitis
AUTHORS: Alison Butler, MD PhD, Michelle Tran, DO, Claudia Alvarez, DO
AFFILIATIONS: Department of Family Medicine, Harbor-UCLA Medical Center
INTRODUCTION: Although ketamine has been known for its anesthetic and psychiatric uses, chronic use of ketamine can lead to both severe hepatobiliary complications and bladder toxicity. This is particularly true when ketamine is used recreationally, which tends to involve higher doses than when used for approved medical indications. We present a case of a 52 year-old male with urinary incontinence and elevated alkaline phosphatase (ALP) who was found to have a history of recreational ketamine use. This case highlights the importance of careful social history-taking and interdisciplinary collaboration.
METHODS: A 52 year-old male was admitted to the family medicine service after being brought in by his sons for concerns about altered mental status. Prior to admission, the patient had been experiencing episodes of loose stool, confusion, and urinary incontinence. Labs demonstrated a leukocytosis of 15.7, ALP of 742, AST of 94, ALT of 128, GGT of 474, and total bilirubin of 1.3. Platelets were 457, INR was 1.25; urine toxicology showed positive for benzos and urine cultures grew ESBL E coli. These lab derangements ultimately prompted consults to multiple specialists. While being interviewed by Addiction Medicine, the patient endorsed using herbal supplements and recreational drugs for the past 37 years, including ecstasy for 24 years and ketamine for the past 6 years. The GI team proposed a diagnosis of DILI but noted the possibility of ketamine-induced sclerosing cholangitis should also be suspected based on the patient's history of heavy use. His liver enzymes down-trended over his hospitalization; he also had a negative PEth test, negative Actin IgG and negative mitochondrial antibodies.
DISCUSSION: This case describes a patient with chronic, heavy ketamine use who presented with urinary incontinence, acute encephalopathy, and elevated liver function tests. Given the modest improvement in his hepatic function while abstaining from ketamine over his admission, it was suspected that his presentation was consistent with a diagnosis of ketamine-induced cholangitis. Ketamine stimulates NMDA receptors in the bile duct smooth muscle, leading to chronic inflammation, fibrosis, and strictures. His ongoing urinary symptoms were likely due to the direct toxic effect of ketamine on the urinary epithelium. This case emphasizes the need for collaboration between specialists in order to identify patients at risk of rare complications from less common types of substance use disorders.
When Both Knees Fail: Simultaneous Bilateral Tibial Tubercle Avulsion Fractures in an Adolescent. A rare case report
AUTHORS: Luis Chaviedo Gutierrez MD (1), Kyung Hwan Kim MD (1), Rachel Battersbersby MSIII (2), Harnek SIngh MD (1)
AFFILIATIONS: (1) Rio Bravo Family Medicine Residency Program; (2) Western University of Health Sciences
INTRODUCTION: Tibial tubercle avulsion fractures are uncommon injuries typically seen in adolescent males during periods of rapid growth, often associated with high-energy quadriceps contraction during athletic activity. Simultaneous bilateral involvement is exceedingly rare, with fewer than 20 cases reported in the literature. Early recognition is essential to prevent long-term functional impairment and optimize outcomes.
METHODS: This case describes a 13-year-old obese male with no significant past medical history presenting after a fall while playing basketball. The patient landed on both knees in flexion after a layup attempt, developing immediate severe bilateral knee pain and inability to bear weight. On examination, both knees were swollen and tender with limited range of motion. The patient was unable to flex or extend the knees, and bilateral patella alta was noted. Neurovascular status was intact. Radiographs showed moderately displaced bilateral tibial tubercle avulsion fractures with intra-articular extension and approximately 1.4 cm anterior displacement. The patient underwent sequential bilateral open reduction and internal fixation. Postoperatively, he progressed with early isometric exercises, gradual range of motion, and progressive weight-bearing. Full weight-bearing was achieved by two months, with significant pain resolution by three months and gradual return to activity.
DISCUSSION: Simultaneous bilateral tibial tubercle avulsion fractures are rare injuries that result in significant disruption of the extensor mechanism. Risk factors include adolescent growth spurts, increased body mass, and high mechanical stress during athletic activities. This case emphasizes the importance of maintaining a high index of suspicion in adolescents presenting with acute bilateral knee pain and inability to ambulate after trauma. Prompt radiographic evaluation and early surgical management are critical to restore function and prevent complications such as extensor mechanism dysfunction or growth disturbances. Early diagnosis, timely intervention, and structured rehabilitation are associated with favorable functional outcomes and safe return to activity.
Double Trouble: Persistent Shoulder Pain in a Young Female
AUTHORS: Sessen Dudek, MD (1) & Amanda Honsvall Hoefler, MD (1,2)
AFFILIATIONS: UCLA Department of Family Medicine (1) & Division of Sports Medicine, Los Angeles, CA (2)
INTRODUCTION: A 29 y.o. female presented with right shoulder pain characterized by heaviness and weakness in the shoulder and intermittent numbness in the hand. She was later diagnosed with Neurogenic Thoracic Outlet Syndrome and Pectoralis Minor Syndrome, together known as Double Crush Syndrome. This case is unique as infraclavicular compression at pectoralis minor is rare and neuromuscular blockade was critical to diagnosis. Additionally, treatment with botulism toxin can be considered in refractory Neurogenic Thoracic Outlet Syndrome.
METHODS: Nine months of persistent shoulder pain despite rest, activity modifications, OTC pain medications, previous formal physical therapy and ongoing home exercises. The pain improves with rest and is aggravated by heavy lifting, working her desk job, driving, and running. Symptoms also occur at night. Denied skin color changes or hand weakness. Right UE: TTP at proximal biceps tendon, anterior/posterior GH joint lines, scalene, pectoralis, and scapular stabilizer musculature. Full ROM. Internal and External Rotation 5-/5 and Abduction 5/5. (+) Neer, O’Brien’s, Yergason, Speed, Adsons, Roos, Cubital Tunnel Tinel, Radial Tunnel Tinel, Carpal Tunnel Tinel and Phalen tests. (-) Spurling's and Hawkin’s. Neurovascular intact. Imaging: Right Shoulder XR: Chronic AC joint injury. C-Spine XR: Straightening of cervical lordosis. Otherwise, normal C-Spine MRI, MR Arthrogram, Right UE EMG/NCS, and MR Right UE Angiogram. Underwent anterior scalene block but endorsed persistent paresthesia with pectoralis minor palpation. 95% relief after subsequent pectoralis minor block.
DISCUSSION: Vascular Surgery was consulted for suspected Thoracic Outlet Syndrome (TOS) despite negative imaging. Positive diagnostic neuromuscular blocks and subsequent symptom recurrence after anesthetic wear-off confirmed the diagnoses of neurogenic TOS and Pectoralis Minor Syndrome. Fluoroscopy guided botulinum toxin injection to the anterior scalene and pectoralis minor resulted in immediate and significant relief. TOS is a neurovascular compression disorder causing paresthesia, weakness, and pain in the upper extremity. Compression typically occurs in the scalene triangle or costoclavicular space, while infraclavicular compression at pectoralis minor is rare. This case demonstrated dual compression at the scalene and pectoralis minor, with neuromuscular blockade proving critical to diagnosis.
Disseminated Intravascular Coagulation as the Initial Presentation of Metastatic Prostate Cancer
AUTHORS: Nina Fukuma, MD (1), Jonathan Rees, MD (2)
AFFILIATIONS: (1) Department of Family Medicine at Kaiser Permanente Los Angeles; (2) Department of Internal Medicine at Kaiser Permanente Los Angeles
INTRODUCTION: Disseminated intravascular coagulation (DIC) is an acquired thrombohemorrhagic disorder characterized by uncontrolled fibrinolysis and consumptive coagulopathy. This creates a cascade that results in organ specific or systemic dysfunction from bleeding and/or thrombosis. Recognition of DIC should prompt an investigation into underlying causes such as sepsis, trauma, or malignancy. We present the case of a patient with bleeding (epistaxis) and multi-organ thrombosis (stroke, NSTEMI, mesenteric ischemia) due to DIC, which prompted the discovery of newly diagnosed metastatic prostate cancer.
METHODS: An 83 year-old male with history of hypertension, atherosclerosis, and alcohol use disorder presented to the ED with 3 weeks of post-prandial abdominal pain associated with 20-pounds unintentional weight loss, secondary to suspected mesenteric ischemia. Acute coronary syndrome from NSTEMI (hs-trop 63 to 3,514) was excluded with cardiac catheterization, which showed CAD including a well-collateralized, occluded circumflex artery. Patient’s hospital course was complicated by recurrent epistaxis, followed by an ischemic stroke, and persistent coagulopathy secondary to acute DIC (fibrinogen <60, d-dimer >20, platelets 89, PT 2.0). This finding prompted the initiation of an extensive malignancy evaluation, including bone marrow biopsy which demonstrated metastatic prostatic adenocarcinoma with neuroendocrine differentiation, bone scan which showed diffuse osseous metastasis, as well as an elevated PSA 342. Given persistent DIC, patient was started on treatment for prostate cancer, including Casodex, Enzalutamide, and Orgovyx, with subsequent resolution of DIC.
DISCUSSION: This patient’s prostate cancer was diagnosed due to the identification of DIC, which manifested as epistaxis and multi-organ infarction (stroke, mesenteric ischemia, and NSTEMI). While uncommon, DIC can be the first clinical manifestation of undiagnosed prostate cancer. In fact, up to 40% of untreated prostate cancer patients may have a degree of subclinical coagulopathy (1). A retrospective analysis correlated the presence of DIC in prostate cancer with disease severity including tumor grade, castrate resistance, and poor prognosis (2). Given that DIC in prostate cancer is a rare complication and associated with high mortality, this case highlights the importance of early identification of underlying prostate cancer in DIC to allow for expedited treatment and reversal of coagulopathies.
Janus-Faced Effect of Insulin Autoantibodies: A Case of Hirata Disease
AUTHORS: Klevin Roger L. Reyes, MD; LeMar Hamilton, MD; Lauren Joseph, MD; Alexandra Rabotin, MD, MPH
AFFILIATIONS: Mission Community Hospital, Department of Family Medicine
INTRODUCTION: Hirata disease, or insulin autoimmune syndrome (IAS), is a rare cause of episodic endogenous hyperinsulinemic hypoglycemia in exogenous insulin-naive patients. [1] While most cases are self-limiting and predominantly reported in East Asian populations, particularly in Japan, IAS can occur across various other ethnic groups. [2] We present a presumptive case in a Hispanic patient with type 2 diabetes (T2DM), highlighting the importance of recognizing IAS in unexplained hypoglycemia, even in ethnicities outside East Asia.
METHODS: A 47-year-old Hispanic male with T2DM presented with recurrent hypoglycemia over 6 months. He was diagnosed with T2DM in June 2025 (A1c 11.3%) at an urgent care and later initiated metformin 500mg BID. At 1-month follow-up, A1c dropped to 6.4%. He reported postprandial tremors, dizziness, diaphoresis, and palpitations 2–3 hours after meals, resolving with oral sugar. Capillary glucose readings during symptoms were consistently <60 mg/dL, nadir 58 mg/dL. He denied other medications, consuming unripe ackee fruit, or metformin misuse. Work-up revealed elevated proinsulin (56.9 pmol/L) and positive insulin autoantibodies (8.3 U/mL); islet cell and GAD antibodies were negative. There was no history of exogenous insulin use, other autoimmune conditions, or renal/hepatic dysfunction. Management focused on dietary modifications: 5–6 small daily meals high in protein and complex carbohydrates with a low glycemic index to minimize insulin spikes. Simple sugars were restricted to acute management. He was referred to endocrinology for suspected Hirata disease.
DISCUSSION: The patient’s recurrent postprandial hypoglycemia, elevated proinsulin, and positive insulin autoantibodies in the absence of exogenous insulin exposure strongly suggest Hirata disease. The autoantibodies are biphasic, they initially bind insulin to induce postprandial hyperglycemia, followed by spontaneous, inappropriate insulin dissociation that triggers severe late-phase hypoglycemia. Although rare in Hispanic populations, Hirata disease can manifest in T2DM idiopathically or via pharmacologic triggers. Diagnosis primarily relies on the presence of insulin autoantibodies. The condition is often self-limiting. Management emphasizes nutritional strategies, mainly frequent, small, low-glycemic meals. Immunomodulatory therapy is reserved for severe or persistent cases.
From Prescription to Dependence: Opioid Use Disorder Following Treatment of a Sports Injury in a Young Athlete
AUTHORS: Kyung Hwan Kim, MD; Luis Chaviedo, MD; Rachel Battersby, OMSIII; Harnek Singh, MD
AFFILIATIONS: Clinica Sierra Vista/ Rio Bravo Family Medicine Program
INTRODUCTION: Opioid analgesics are commonly prescribed for acute sports injuries, but even short-term use can increase the risk of opioid use disorder (OUD), particularly in young athletes. Pressure to maintain performance and return to play may contribute to prolonged use. This case highlights progression from appropriate opioid prescribing for a sports injury to OUD, emphasizing the need for cautious prescribing, patient education, and early recognition of misuse
METHODS: A 20-year-old male baseball athlete with no prior medical history sustained a right shoulder injury and was prescribed hydrocodone/acetaminophen. He initially used the medication as directed but continued due to persistent pain affecting performance. Over time, he escalated use beyond prescribed doses. After discontinuation, he obtained opioids from non-prescribed sources, including oxycodone and fentanyl, leading to opioid dependence and multiple failed cessation attempts. Six months after the initial injury, he presented for treatment. Medication-assisted therapy with buprenorphine/naloxone was initiated along with behavioral counseling and urine drug monitoring. Follow-up showed adherence, absence of illicit opioid use, improved functioning, and resolution of cravings. The patient successfully returned to baseball without opioid use.
DISCUSSION: This case highlights the risk of progression to OUD following opioid prescribing for sports injuries in young athletes. Performance pressure may contribute to prolonged or escalating use. Clinicians should prioritize non-opioid therapies such as NSAIDs and physical therapy, and when opioids are necessary, prescribe the lowest effective dose for the shortest duration. Early identification of misuse is critical. Medication-assisted treatment with buprenorphine/naloxone is effective for recovery and functional restoration, enabling return to normal activities, including athletics.
A Painful Twist on Pseudogout: A Case Report of Atypical Hyperalgesia
AUTHORS: Jasmine Nevarez, MD, MSPH (1), Bernadette Pendergraph, MD (2)
AFFILIATIONS: (1) Harbor-UCLA Family Medicine; (2) Harbor-UCLA Family Medicine, Team to Win, Kaiser Permanente Sports Medicine Fellowship
INTRODUCTION: Calcium Phosphate Deposition Disease (CPPD), or Pseudogout typically presents similarly to gout: a painful, erythematous joint with effusion. In this case, a 71-year-old patient presented for syncope provoked by acute onset exquisite left knee pain, with an initial exam with trace effusion and hyperalgesia. This case highlights an unusual presentation of CPPD with progression of symptoms during hospitalization and the importance of expedited work up to rule out septic joint with appropriate laboratories, imaging, and arthrocentesis.
METHODS: A 71-year-old previously ambulatory female with a history of CAD, diabetes, and calcific mitral stenosis presented to the ED for presyncope evoked by severe left knee pain that made her faint. She had no prior episodes, was not able to bear weight in the ED, and no recent infections. Initial left knee exam was significant for hyperalgesia, small non warm effusion, no erythema, and limited motion. Left knee xray showed small effusion, mild degenerative changes, and no fracture. ESR was 90, CRP was 150, and the rest of the labs were normal. Over the course of admission, both knees had more effusion and warmth. Given limitations in exam, CT scans were obtained which showed a large effusion and a 4mm calcification near the lateral meniscus consistent with chondrocalcinosis. Rheumatology assisted with an arthrocentesis which showed rhomboid crystals, white blood cells of 10,848, and negative culture confirming pseudogout. Steroid injection helped with the knee pain. Colchicine could not be started for her pseudogout as she was on amiodarone for new onset atrial fibrillation.
DISCUSSION: This was an unusual presentation of CPPD, presenting with knee hyperalgesia and syncope. CPPD acute flares generally are less intense than gout flares, and present with a warm, swollen joint. Arthrocentesis is key to confirming the diagnosis and ruling out infection but chondrocalcinosis can be seen on x-rays with calcium deposition in cartilaginous structures such as meniscus that can support the diagnosis. Pseudogout like gout has acute onset of pain but may last several weeks instead of the more limited course expected with gout. Colchicine is used to treat acute flares as well as prophylaxis. Comorbid conditions can limit treatment choices. In this case, rheumatology recommended prophylaxis with colchicine which cannot be used if the patient is taking medications such as amiodarone.
Early-Onset Psoriasis in a Toddler Initially Misdiagnosed as Recurrent Bacterial Skin Infection
AUTHORS: Daniel Zumerkorn Hassan, MD; Ninelle Zargarian, DO; Klevin Roger Reyes, MD; Atoosa Shahriari, MD; Petros Hajian, DO
AFFILIATIONS: Mission Community Hospital, Panorama City - California
INTRODUCTION: Psoriasis in toddlers is uncommon and may present atypically, leading to misdiagnosis. We present a 3-year-old male with a chronic progressive rash initially treated multiple times as bacterial skin infection without improvement. Biopsy later confirmed psoriasis. This case highlights the importance of reconsidering the diagnosis in children with persistent rash unresponsive to antibiotics and the role of biopsy in establishing the diagnosis.
METHODS: A 3-year-old male presented with a chronic progressive rash beginning as erythematous papules on the lumbosacral region that spread to the trunk, face, scalp, extremities, and genital area. He was treated with ketoconazole, clindamycin, and trimethoprim-sulfamethoxazole for presumed fungal and bacterial infections without improvement. Dermatology initially suspected pityriasis lichenoides and treated with erythromycin and later oral steroids. Skin biopsy demonstrated spongiotic and psoriasiform dermatitis with intracorneal neutrophils, consistent with psoriasis. The patient was treated with systemic and topical corticosteroids with significant clinical improvement and residual hypopigmented macules.
DISCUSSION: Psoriasis in young children may present atypically and mimic infectious skin conditions such as impetigo or ecthyma, leading to delayed diagnosis and unnecessary antibiotic use. This case demonstrates the importance of reconsidering the diagnosis in pediatric patients with rash unresponsive to antimicrobial therapy. Skin biopsy can help confirm psoriasis when clinical presentation is unclear. Early recognition and dermatology referral can reduce unnecessary treatments and improve outcomes.
Joshua Tree Room - Abstracts
Repeat Participation and Produce Utilization in a Safety-Net Food Prescription Produce Distribution Program
AUTHORS: Frederick Ferguson MD MS (1); Michael Baham, MD (1); William McCarthy, PhD (2); Arleen Brown, MD PhD (3,4); Alejandra Casillas, MD MSHS (3,4); Stefanie Vassar (3,4); Julia Caldwell, MPH PhD (5); Fatinah Darwish-Elsherbiny, MPH RDN (5); Tony Kuo, MD MSHS (1,6,7,8)
AFFILIATIONS: (1) Department of Family Medicine at UCLA; (2) Department of Health Policy and Management, UCLA Fielding School of Public Health; (3) Disparities Elimination through Coordinated Interventions to Prevent and Control Heart and Lung Disease Risk (DECIPHeR) Alliance at UCLA; (4) Division of General Internal Medicine and Health Services Research at UCLA; (5) Nutrition and Physical Activity Program, Division of Chronic Disease and Injury Prevention, Los Angeles County Department of Public Health (LAC DPH); (6) Department of Epidemiology, UCLA Fielding School of Public Health; (7) Population Health Program, UCLA Clinical and Translational Science Institute; (8) Division of Chronic Disease and Injury Prevention, LAC DPH
INTRODUCTION: Food insecurity and diet-related disease disproportionately affect low-income populations. Clinic-based produce distribution programs increase access to fruits and vegetables, yet utilization remains variable. Food neophobia and limited resources may deter households from using unfamiliar, minimally processed foods. Prior research links repeat participation to improved intake, but mechanisms are unclear. This study examines whether repeat attendance is associated with produce utilization and explores barriers to full consumption.
METHODS: We conducted a secondary analysis of cross-sectional survey data from 451 English- and Spanish-speaking adults attending FoodRx clinic-based produce distribution events in Los Angeles County. Returning participants (≥2 prior visits) were categorized by attendance (2–3 vs ≥4 visits). The primary outcome was self-reported consumption of all produce (yes/no). Covariates included food security (USDA 6-item), age, sex, Hispanic origin, SNAP participation, chronic conditions, and household size. Chi-square tests assessed associations between attendance and consumption.
RESULTS: Among 451 participants, 368 reported repeat attendance; 58% consumed all produce and 33% consumed less than all. Attending ≥4 events was associated with higher full consumption compared to 2–3 visits (69% vs 31%, p=0.002; adjusted OR=2.38, 95% CI: 1.43–3.95). Larger households were more likely to consume all produce (82% vs 69%, p=0.002). SNAP participation was associated with lower odds of full consumption (OR=0.46, 95% CI: 0.26–0.83). Demographics, food security, and chronic conditions were not significant. Barriers included poor quality (21.7%), limited preparation knowledge/equipment (13.9%), excess quantity (11.1%), and time constraints (3.9%).
CONCLUSIONS: In this secondary analysis of cross-sectional survey data, greater exposure to FoodRx produce distributions was associated with improved produce utilization. However, practical and behavioral barriers—including food quality concerns, limited preparation knowledge, and lower utilization among SNAP participants—persist. Findings highlight the need for community informed strategies, including culturally responsive nutrition education, cooking support, and recipe sharing, to reduce waste and improve dietary quality in underserved populations.
Protecting Patient Rights in a Worsening Immigration Enforcement Landscape: Advancing Healthcare Worker Training and Health Facility Model Policy
AUTHORS: Abhinaya Narayanan, MD, MPP (1); and Matthew Hing, MD/PhD Candidate (2)
AFFILIATIONS: (1) Harbor-UCLA Department of Family Medicine; and (2) David Geffen School of Medicine at UCLA
INTRODUCTION: Across LA County and the country, we have seen a dramatic rise in patients being brought into health facilities in immigration custody after brutalization at the hands of officers in the course of detention or medical neglect in detention facilities. As a result, healthcare workers encounter conflict with immigration enforcement officials and violations of basic patient privacy and legal rights. This ongoing community project and policy endeavor aims to establish and implement a model policy that protects the rights of patients in civil immigration custody.
METHODS: We developed a working group to evaluate medical legal expertise and promote dissemination of best practice guidelines for clinicians caring for immigrant communities and patients in civil immigration custody. We conducted a scoping review of healthcare forensic policies across the medical literature and professional society guidelines, bioethical frameworks, and relevant local, state, and federal laws. The physician working group expanded to include legal experts, bioethicists, and human rights experts at the California Immigrant Policy Center, American Civil Liberties Union, Immigrant Defenders Law Center, among many others and co-authored a model policy that underwent review by legal, human rights, and labor experts to ensure compliance with existing legal and regulatory requirements.
RESULTS: This model policy has been disseminated and used to inform policy at multiple health systems, including a new policy at LA County Department of Health Services. Ongoing challenges remain as we continue to see barriers in timely access to attorneys while in the hospital, violations of patient privacy, healthcare workers facing restrictions in calling family members of detained patients, and tensions between frontline workers and hospital administrators. Members of the working group have been providing training on best practices to healthcare workers based on the model policy to fill these gaps. In addition SB 915, informed by the model policy, is moving through the state legislature and would require a uniform minimum standard for the rights of patients in immigration custody.
CONCLUSIONS: This immigration policy and education project has served to provide a framework for how the lived experiences of healthcare workers on the frontline can be used to inform model policy and best practices that advance the well-being and safety of our immigrant patient communities.
Improving Clinic Cycle Time and Team-Based Efficiency Through Agenda Setting in an Ambulatory Resident Clinic: Resident Self-Efficacy Perspectives
AUTHORS: Nancy Rodriguez, MD, MPH, MBA, MHA; Jocelyn Shorts MD, MPH, MSc; Omar Khaled, MD; Kevin Kemp II, MD; Mayra Duran, MD; Matthew Yu, DO, MPH, DipABLM, FAAFP; Karamjit Chela, MD, MPH
AFFILIATIONS: Department of Family Medicine at Charles R. Drew University of Medicine and Science, LAC-DHS Martin Luther King Jr. Outpatient Center
INTRODUCTION: Agenda setting the practice of eliciting a patient’s full list of concerns and collaboratively prioritizing visit goals, is a teachable communication skill associated with fewer end-of-visit surprise concerns and improved encounter efficiency. Despite its relevance to ambulatory care, it is infrequently taught as a formal component of family medicine residency curricula. Baseline observational data at our institution identified resident encounter duration as a major contributor to prolonged cycle time, with PGY2 residents demonstrating the longest mean encounter times, suggesting communication efficiency is a distinct and teachable competency.
METHODS: This prospective pre/post survey study included all PGY-1, PGY-2, and PGY-3 family medicine residents (estimated n=20–25). Residents completed an 8-item Likert-scale self-assessment before the intervention (April 2026) and approximately three weeks after a structured agenda-setting workshop (late April–early May 2026). Survey domains included knowledge of agenda-setting principles, competence in four behavioral components (concern elicitation, priority negotiation, communication of visit scope, and perceived time cost), and overall confidence. Subgroup analyses will compare responses by PGY year. This is one of four companion QI studies evaluating the same intervention alongside faculty, nursing, and objective cycle-time measures.
RESULTS: Data collection is ongoing. Pre-intervention survey findings will be presented alongside baseline cycle-time data from two observed clinic weeks. Baseline data demonstrated a 54-minute intra-cohort cycle-time range among PGY-1 residents attending the same clinic session with identical preceptors, suggesting substantial individual-level variation beyond training year or clinic structure alone. These findings support the need for targeted communication skills training. Post-intervention survey data, including changes in self-rated knowledge, competence, and confidence, will be available at the time of presentation.
CONCLUSIONS: Resident self-efficacy outcomes are most meaningful when interpreted alongside external measures such as faculty perceptions and cycle-time data. Alignment between improved resident confidence, observed communication behaviors, and shorter encounter times would provide stronger evidence of meaningful practice change. These findings may help identify training-year specific educational needs and inform whether longitudinal reinforcement is required to sustain communication skill development.
Teaching to Learn: A Resident-Led Musculoskeletal Ultrasound Outreach Curriculum and Its Impact on Resident Teaching Confidence
AUTHORS: Alexander Soto MD, MPH (1,2); Jeffery Ezennia MD, MS (2); Sessen Dudek MD (2); Spencer McCaffrey, MD (2); Annie Hernandez, MD, MPH (2); Calvin Duffaut (1,2)
AFFILIATIONS: (1) Department of Sports Medicine at UCLA; (2) Department of Family Medicine at UCLA
INTRODUCTION: Musculoskeletal point-of-care ultrasound (MSK-POCUS) is increasingly incorporated into residency training, yet opportunities for residents to develop teaching skills in imaging-based education remain limited. Near-peer teaching may reinforce knowledge while simultaneously developing residents as educators. We implemented a community-engaged curriculum in which residents taught MSK ultrasound concepts to high school students and evaluated its impact on resident teaching confidence.
METHODS: Family medicine residents served as volunteer instructors in a structured musculoskeletal ultrasound session for high school students through a community pipeline program. Residents were provided standardized preparatory materials, including a teaching outline, instructional videos, and slides covering ankle anatomy, physical examination, and introductory ultrasound techniques. Participants completed anonymous pre- and post-session surveys assessing overall teaching confidence (0–100 scale) and specific competencies (physical exam instruction, ultrasound scanning, explaining anatomy, and responding to questions). Surveys were paired using self-generated codes. This was conducted as an educational quality improvement initiative within the residency curriculum.
RESULTS: Participants were UCLA Family Medicine residents involved in a high school musculoskeletal ultrasound teaching experience. Paired t-tests showed statistically significant improvements in confidence for ankle physical exam (Δ +1.75, p=0.006, d= 3.5), ankle ultrasound technique (Δ+1.75, p=0.035, d= 1.8), explaining anatomy/pathology (Δ+1.75, p= 0.006, d=1.83), and answering learner questions (Δ+1.50, p= 0.014, d= 2.6). Creating a positive learning environment demonstrated improvements, but was not statistically significant (Δ +0.75, p = 0.058, d=1.50). Overall teaching confidence (Δ+18.75, p = 0.036, d=1.82) also improved, with gains across all PGY levels.
CONCLUSIONS: Our study suggests the feasibility and efficacy of implementing near-peer teaching of MSK POCUS within FM resident education. Participants reported increased confidence in teaching and explaining MSK POCUS techniques, anatomy, and common pathologies. Limitations include small sample size, and single-institution design, limiting generalizability. Although exploratory, the study achieved a 100% response rate. Overall, this study demonstrates that near-peer teaching can be incorporated into resident education and may significantly improve resident confidence in MSK anatomy and POCUS skills.
Hemoglobin A1C Before and After Holidays in Patients with Type 2 Diabetes Mellitus
AUTHORS: Javier Torres, MD, and Cindy Yang, MD
AFFILIATIONS: Dignity Health Northridge Family Medicine
INTRODUCTION: The holiday season is associated with changes in diet, physical activity, and routine,potentially worsening glycemic control in patients with DM2. Previous studies have noted seasonal fluctuations in metabolic markers, but limited research focuses specifically before and after the holidays period. This study builds on that gap to assess changes in HbA1C across two time points. This retrospective observational study investigates the effects of the holiday season on glycemic control in patients with Type 2 Diabetes Mellitus (DM2). Specifically, it evaluates changes in hemoglobin A1C (HbA1C) levels before and after the holidays period.
METHODS: Study Type: Retrospective cohort study. Setting: Dignity Health Family Medicine Clinic at Northridge. Timeline: Pre-holiday HbA1C: Sep–Nov; Post-holiday HbA1C: Jan–Mar. Years 2024-2025. Procedures: EMR data extraction of HbA1C values. Study duration: Estimated 3-4 months for data extraction and analysis. DATA COLLECTION - Design: Retrospective chart review. Data Source: Electronic Medical Records (CERNER). Data Collected: - HbA1C pre- and post-holidays. - Age, sex.
RESULTS: A paired t-test was conducted to evaluate whether there was a statistically significant difference in hemoglobin A1C levels before and after the holidays season among patients included in the study. A total of 52 paired observations were analyzed. The mean pre-holiday A1C was 7.99% (SD = 1.97), while the mean post-holiday A1C was 7.55% (SD = 1.67). The analysis demonstrated a mean reduction of 0.44% in A1C levels following the holiday period. The paired t-test indicated that this difference was statistically significant, t (51)= 2.36, p = 0.022 (two-tailed). The Pearson correlation between pre- and post-holiday A1C measurements was r = 0.73, indicating a strong positive relationship between the paired observations.
CONCLUSIONS: This retrospective study evaluated changes in hemoglobin A1C levels before and after the holiday season among patients with Type 2 Diabetes Mellitus. Contrary to the initial hypothesis, which anticipated worsening glycemic control during the holiday period, the results demonstrated a statistically significant reduction in mean HbA1C levels following the holidays. The mean HbA1C decreased from 7.99% pre-holidays to 7.55% post-holidays, representing an average reduction of 0.44% (p = 0.022). These findings suggest that glycemic control did not worsen during the holidays season.
Improving Pediatric Dental Health: A QI Project to Increase Fluoride Varnish Application Rates in a Primary Care Setting
AUTHORS: Amanda Tran, MD; Melissa Gee, MD; Anita Wong, MD; Blanca Hernandez, MD
AFFILIATIONS: University of California, Los Angeles Department of Family Medicine
INTRODUCTION: The prevalence of dental caries in all children is >40%, and even higher prevalence is seen in low socioeconomic and minority groups. Studies have shown that fluoride varnish (FV) application is an effective therapy to prevent caries. Consequently, professional associations recommend that primary care providers include dental assessments, parent education, and FV application in well-child visits. Despite this, providers have anecdotally underused FV at the Mid-Valley Clinic, which serves low-income and minority groups. Thus, this QI project aims to address barriers to and increase application of FV for children at this county clinic.
METHODS: A chart review of 6-month to 5-year-old well-child checks was conducted during a 6-month pre-intervention period (6/01/2025-12/31/2025) to evaluate potential barriers to and baseline rates of FV application. In 1/2026, an intervention to address these barriers was implemented and included: an educational presentation for providers about FV need and indications; staff training on applying FV; informative dental handouts for parents; and a standardized FV protocol delineating the workflow and responsibilities of providers (confirmation of FV eligibility and parent education) vs. staff (consent, order entry, and application). A preliminary post-intervention chart review (2/1/2026-4/17/2026) was conducted to determine whether there was an increase in FV application and a decrease in barriers.
RESULTS: FV application rates quantitatively increased after intervention implementation. FV was given to 40% (25/62) of eligible patients in the pre-intervention period, and 56% (23/41) of eligible patients in the post-intervention period. There was also a quantitative decrease in certain barriers after intervention implementation. Namely, providers' inadequate education (13% -> 0%), deferral to the patient's established dentist (40% -> 11%), and time constraints (24% -> 5%) were less frequently cited as reasons why FV was not given to eligible patients. However, there was an increase in the percentage of parent declination (5% -> 50%) and non-cooperative patients (2% -> 12%) from the pre- to the post-intervention period.
CONCLUSIONS: This multi-pronged project increased FV application rates. Thus, integrating this into routine care can expand delivery of a proven therapy to prevent caries in high-risk children. Preliminary results suggest that the intervention's strengths are streamlining workflows and educating providers. However, the higher percentage of parent declination highlights parent education as a possible weakness. Data will be collected until 7/31/2026. Next steps include surveys to evaluate providers' knowledge of FV guidelines, staff's outlook on protocol sustainability, and parents' attitudes towards FV.
Hear Us Out: Educating Residents on Hearing Loss and Hearing Assistive Tools in the Clinical Setting
AUTHORS: Kaycee Ching, MD, Nina Fukuma, MD, Melody Wang, MD, Jeegar Rana, MD
AFFILIATIONS: Department of Family Medicine, Kaiser Permanente Los Angeles Medical Center
INTRODUCTION: Age-related hearing loss (presbycusis) is common and progressive in older adults and is linked to cognitive impairment, dementia, and late-life depression. In the US, over 63% of adults ≥70 and >80% of those ≥80 have hearing loss, yet fewer than 20% receive treatment. Hearing loss remains prevalent and undertreated, highlighting the need for improved clinical management.
METHODS: We conducted a two-part quality improvement project to enhance communication with hearing-impaired patients in clinic and inpatient family medicine settings. Five Pocketalker devices were acquired and made accessible. Family medicine residents (PGY1–PGY3) attended a session covering hearing loss epidemiology, risk factors, screening, introduction to Pocketalker devices with hands-on practice, and evidence-based communication strategies, including clear speech and confirming understanding. Pre- and post-session surveys assessed residents’ confidence and device use.
RESULTS: Pre- (n=17) and post-intervention (n=14) responses were compared using chi-squared and t-tests. Residents showed significant gains in all knowledge measures, including knowledge of addressing hearing loss (p < 0.001) and pocket talkers (p = 0.035), and awareness of clinic and hospital hearing-assistive devices (p < 0.001). Communication effectiveness improved (p < 0.001, Cohen’s d = 1.57), and perceived helpfulness increased (p = 0.025). Confidence showed non-significant overall gains, though PGY-1 and PGY-2 residents improved significantly (p = 0.025, p = 0.009) while PGY-3 residents did not (p = 0.095). Post-intervention scores did not differ across PGY levels, suggesting the intervention leveled confidence. Interest in learning and perceived need for sound amplifiers remained high.
CONCLUSIONS: The intervention significantly improved residents’ knowledge, awareness of resources, and communication effectiveness. Nearly half of the surveyed group initially lacked knowledge of assistive hearing devices, highlighting the importance of trainee education to remove barriers to patient communication. Variability in confidence gains suggests knowledge alone may not translate to confidence in communication, therefore experiential learning may be needed. The intervention leveled performance across resident trainee levels and supports broad adoption in residency programs.
Enrollment Characteristics and Barriers in a Large Randomized Controlled Trial for Sinusitis
AUTHORS: Christopher Whitlock, MD; Hannah M. Cummins, MD, MPH; Daniel T. Lee, MD; Danielle Schramm, MSPH; Aika O. Misawa, MA; Genesis De La Rosa, Simone J. Riley, Stella Shebat, Felicity Nguyen, Jonathan Wu, Kaylee Hsieh, Emely Gonzalez, and Derjung M. Tarn MD, PhD
AFFILIATIONS: Department of Family Medicine at UCLA
INTRODUCTION: Acute rhinosinusitis (ARS) afflicts one in seven adults every year in the United States. Though most cases are viral, antibiotics are prescribed in over 70% of clinician visits without clear benefit to patients. The Nasal Irrigation, Oral Antibiotics, and Subgroup Targeting for Effective Management of Acute Sinusitis (NOSES) study seeks to improve ARS management. The NOSES trial is a large, randomized, controlled trial in primary and urgent care clinics across six geographical regions. This study elucidates differences between enrolled and nonenrolled participants in one geographic area of the trial and identifies enrollment barriers.
METHODS: This is a cross-sectional analysis of patients screened for participation in the NOSES clinical trial. Eligible participants were English- or Spanish-speaking patients aged 18-75 years old with any acute upper respiratory symptoms for fewer than 21 days. Patients with penicillin allergies and antibiotic use in the past month were excluded. We compared demographics of eligible enrolled and nonenrolled patients using t-tests or chi-square analysis as applicable and performed multivariable logistic regression models to evaluate associations between demographic characteristics, clinical trial enrollment, and reasons for refusal if patients declined to enroll.
RESULTS: Of 312 eligible patients, 58% (n=181) enrolled in the trial. Enrolled patients were younger than nonenrolled paitents (mean age 43.6 (SD=14.8) vs 50 years (SD=15.2), p<0.001) and more likely to identify as a non-White race (50% vs 37%, p<0.05). There was no significant difference in the distributions of sex or ethnicity between groups. Multivariable logistic regression showed increasing age was associated with lower odds of enrollment [OR = 0.97 (95% CI (0.95 - 0.99)], while race was not an independent predictor of enrollment. Among 263 patients who reported reasons for nonenrollment, the most common were time constraints (17%) and concerns about receiving placebo treatment (16%).
CONCLUSIONS: Patients who enrolled in the NOSES clinical trial were significantly younger compared to nonenrolled patients, and reported barriers to enrollment included time constraints and concerns about placebo treatment. This study highlights the need for continued efforts to increase enrollment of older adults and for strategies to address major patient barriers to enrollment.
Improving Resident Satisfaction with Feedback Using a Mobile Real-Time Feedback Application in a Family Medicine Residency
AUTHORS: Anita Wong MD; Thalia Nguyen MD; and Frederick Ferguson MD MS
AFFILIATIONS: Department of Family Medicine at UCLA
INTRODUCTION: Formative feedback, defined as low-stakes, timely, and specific feedback intended to guide learner improvement, is a cornerstone of competency-based medical education (CBME). Feedback theory emphasizes its role in promoting deliberate practice and progression towards competency. However, residents frequently report receiving delayed and nonspecific evaluations that limit learning. In our residency, baseline data revealed gaps in feedback frequency, timeliness, and specificity. We implemented use of a mobile feedback application (myTIPreport) to improve the quantity and quality of formative feedback provided to residents.
METHODS: We conducted a mixed-methods pre-post study in a university-based family medicine residency. Baseline surveys were completed by 25 of 36 residents (70%) and 8 of 24 faculty (33%), assessing feedback frequency, timeliness, specificity, and satisfaction. The intervention introduced myTIPreport, a mobile app that integrates with existing evaluation systems (Medhub). The myTIPreport app enables faculty preceptors to enter rapid (~1 minute), point-of-care, and objective feedback immediately after observing a resident encounter. Residents and core faculty were trained on use of the app through didactic sessions and faculty development. Core faculty members will undergo additional faculty development on providing effective feedback and incorporating direct observation in clinic efficiently.
RESULTS: At baseline, 56% of residents reported receiving feedback only a few times per month, and 24% received timely weekly feedback. Feedback lacked specificity (68% somewhat specific; 12% not specific), with moderate satisfaction (3.48/5 quantity; 3.40/5 quality). While all faculty reported providing verbal feedback and high comfort (4.0/5), only 25% did so consistently during clinical encounters. Following implementation of the myTIPreport app, 21/36 residents (58%) and 8/18 faculty (44%) completed ≥1 evaluation in a two month period. Of 35 evaluations requested, 26 (74%) were completed, all within 2 weeks (100%). Early use demonstrates feasibility and improved timeliness, though challenges remain in faculty adoption, workflow integration, and competency navigation.
CONCLUSIONS: Implementation of a mobile feedback platform is feasible and addresses key workflow barriers to timely, specific feedback. Early experience demonstrates strong potential to improve feedback quality and resident experience. Ongoing efforts include additional faculty development on observation and providing feedback, and incorporation of resident and faculty feedback of the app to streamline usability, enhance faculty engagement, and optimize integration into clinical workflows. This will ideally support long-term sustainability and broader adoption across training settings.
Joshua Tree Room - Case Reports
Bilateral Optic Neuritis as the Initial Presentation of Acute HIV Infection in a Young Bodybuilder
AUTHORS: Jennifer Lu, DO, Kathleen Tor, MD, Joseph Yasmeh, MD, and Monique George, MD
AFFILIATIONS: Kaiser Permanente Woodland Hills Family Medicine Residency Program
INTRODUCTION: Optic neuritis, an inflammatory demyelinating condition affecting the optic nerve, is typically associated with multiple sclerosis but may reflect systemic disease. Bilateral presentations are uncommon and warrant broader evaluation. We report a 38-year-old man with acute bilateral optic neuritis as the initial manifestation of HIV infection. This case highlights the importance of considering infectious etiologies, including HIV, in atypical or bilateral optic neuritis.
METHODS: A 38-year-old male actively engaged in bodybuilding, anabolic steroid use, and high-risk sexual behavior presented with one week of progressive right-sided vision loss, headache, photophobia, and new left eye color vision changes. Exam showed a visual acuity of OD 20/200 and OS 20/40 with a minimally reactive right pupil. MRI of the brain and orbits demonstrated bilateral optic nerve T2 hyperintensities, consistent with optic neuritis. CSF analysis revealed lymphocytic pleocytosis but negative bacterial, viral, and fungal studies and a negative multiple sclerosis panel. MOG and AQP4 antibodies were negative. HIV-1 testing was positive, confirming new infection, and the optic neuritis was attributed to HIV after exclusion of other etiologies. CTA revealed severe intracranial stenoses, likely related to anabolic steroid use, and the patient was started on aspirin and atorvastatin. For his optic neuritis, the patient was treated with IV methylprednisolone for 5 days with visual improvement. Antiretroviral therapy was also initiated. He was discharged with multidisciplinary follow-up.
DISCUSSION: Bilateral optic neuritis, especially in the absence of established multiple sclerosis or opportunistic infection, is uncommon and should prompt evaluation for systemic causes, including HIV. Although a less recognized etiology, HIV-associated optic neuritis may result from immune-mediated or direct viral mechanisms. Early diagnosis is critical, as timely corticosteroid therapy and antiretroviral treatment can improve outcomes. This case highlights the importance of maintaining a broad differential in atypical presentations of optic neuritis and recognizing HIV as a potential cause of neurologic complications, even in the absence of systemic symptoms.
A Scope Gone Septic: When EGD Takes an Unexpected Turn
AUTHORS: Fatima Maqsood, DO; Adolfo Aguilera, MD
AFFILIATIONS: Riverside University Health System/UC Riverside Family Medicine Residency Program
INTRODUCTION: Transient bacteremia, the temporary presence of bacteria in the bloodstream and cleared by the immune system without causing symptoms, is not uncommon following an esophagogastroduodenoscopy (EGD). However, sepsis is rare. In patients who are immunocompromised or otherwise critically ill, normal gastrointestinal flora can translocate and act as opportunistic pathogens. Such patients are at increased risk of severe infections from such routine procedures as an EGD. Here we present a rare case of sepsis secondary to bacteremia in the setting of bacterial translocation from an EGD.
METHODS: A 54-year-old female with past medical history of decompensated alcoholic cirrhosis and systemic lupus erythematosus (SLE) presented to the ED with fevers, headache, and nausea. She was admitted for sepsis of unclear etiology and started on broad spectrum antibiotics. Urinalysis was negative, chest x-ray was not concerning for pneumonia, respiratory spotfire was negative, no abdominal distension or ascites noted on evaluation to suggest SBP. Lumbar puncture was attempted but unsuccessful, although patient had negative Brudzinski/Kernig sign and no neck stiffness. Blood cultures resulted 2 out of 2 positive for gram positive cocci in chains and ultimately speciated for Streptococcus mitis and Streptococcus oralis. Given that patient had an EGD 2 days prior to admission and developed symptoms within 24 hours of her EGD, the source of her bacteremia was presumed to be a GI translocation event in the setting of her scope. With negative repeat cultures and low suspicion for endocarditis, patient was discharged on oral levofloxacin to complete a 2 week antibiotic course.
DISCUSSION: Transient, asymptomatic bacteremia is a well-documented occurrence with EGD’s and a wide variety of other procedures. Sepsis due to bacteremia following an EGD however, is rare. Immunocompromised patients are at higher risk of such complications. Multiple risk factors, including cirrhosis associated immune dysfunction and immune dysregulation from SLE, can lead to greater susceptibility to bacterial translocation. In such patients, normal GI flora, such as Streptococcus mitis and Streptococcus oralis can present as opportunistic pathogens. For patients with risk factors presenting with sepsis, translocation from procedure should be considered as a possible source and can guide workup and adequate antibiotic coverage.
Ascites of unknown origin. A rare presentation of Disseminated Coccidioidomycosis
AUTHORS: Milanes Bernardino MD; Avila Jessica MD; Hlaing Su MD; Rubio Mariano MD; De Luna Patrick MD; Almnini Nariman MD; Urbina Jose MD; Garcia Stephanie MD
AFFILIATIONS: Rio Bravo Family Medicine Residency Program
INTRODUCTION: Coccidioidomycosis is an endemic fungal infection in the Southwestern United States that typically presents as a self-limited pulmonary illness; however, dissemination can occur, particularly in high-risk or exposed individuals. Extrapulmonary involvement most commonly affects the skin, bones, and central nervous system, while peritoneal involvement remains rare and poorly characterized [1,8]. Peritoneal coccidioidomycosis can mimic malignancy or spontaneous bacterial peritonitis (SBP), creating significant diagnostic challenges [3,4].
METHODS: A 35-year-old immunocompetent male with type 2 diabetes mellitus and nonalcoholic fatty liver disease presented with progressive abdominal distension and recurrent ascites. Initial evaluation demonstrated large-volume ascites requiring repeated paracenteses (up to 7.8 L). Ascitic fluid analysis revealed low serum-ascites albumin gradient (SAAG ~0.5), high protein (~6.2 g/dL), and elevated polymorphonuclear cells (>250 cells/µL), initially raising concern for SBP; however, cultures remained negative. Imaging revealed a spiculated right upper lobe pulmonary nodule. Cytology of ascitic fluid showed lymphocytes, macrophages, and mesothelial cells without malignancy. Peritoneal biopsy demonstrated necrotizing granulomatous inflammation, with negative PAS, GMS, and AFB stains. Serum Coccidioides complement fixation (CF) titer was 1:128. Fungal culture from peritoneal biopsy yielded organisms consistent with Coccidioides species, and peritoneal fluid serology demonstrated reactive IgG with CF titer of 1:256, confirming active peritoneal infection. High-dose fluconazole was started.
DISCUSSION: Peritoneal coccidioidomycosis is a rare manifestation of disseminated disease, with limited cases described in the literature [2–4]. This case illustrates a diagnostic pitfall in which low-SAAG, high-protein ascites with neutrocytosis mimics SBP while lacking portal hypertension. The presence of granulomatous inflammation, negative cytology, and high complement fixation titers were key to diagnosis. Notably, fungal stains may be negative due to low organism burden, necessitating culture and serologic correlation. Elevated CF titers correlate with disease burden and dissemination [8]. Current management guidelines recommend prolonged azole therapy, with escalation to amphotericin B in severe or refractory cases [5,9.
Adult-Onset Still's Disease Following Seasonal Coronavirus Infection in a 65-Year-Old Woman
AUTHORS: Nicolette Mojica-Conklin, MD MPH; Denise Sur, MD; and Paula Trepman, MD MPH
AFFILIATIONS: UCLA David Geffen School of Medicine, Department of Family Medicine
INTRODUCTION: Adult-onset Still's disease (AOSD) is a rare systemic inflammatory disorder characterized by spiking fever, arthralgias and myalgias, evanescent rash, and often hyperferritinemia. Diagnosis of this rare disease is complicated by its low prevalence and incompletely understood pathogenesis. This case highlights AOSD in an older adult outside of the typical bimodal peak of 15–25 and 36–46 years of age following a presumed viral trigger of seasonal coronavirus.
METHODS: A 65-year-old woman with prediabetes developed a prodrome of sore throat, fevers, chills, and night sweats, followed by persistent fevers, myalgias, arthralgias, and a generalized maculopapular rash sparing the face and palms. Exam revealed left knee monoarthritis with swelling. Labs were notable for WBC 19.5, HGB 11.5, ESR 88, CRP 21.9, and ferritin 2779. Infectious workup was positive for seasonal coronavirus; COVID-19, influenza, RSV, mononucleosis, and streptococcal testing were negative. A positive rickettsial IgG (1:64) prompted infectious disease consultation and empiric doxycycline, without resolution. She was initially thought to have reactive arthritis and improved with NSAIDs, however she remained symptomatic for weeks post-discharge and pain became refractory to NSAIDs, thus prednisone was started in the primary care setting. Outpatient rheumatology confirmed AOSD by Yamaguchi criteria (fever ≥1 week, arthralgia ≥2 weeks, maculopapular rash, leukocytosis >10k with neutrophilia, sore throat, elevated inflammatory markers) and initiated methotrexate.
DISCUSSION: AOSD should be considered in patients presenting with arthralgia, myalgia, rash and elevated ferritin after viral infection, regardless of age, to prevent delays in immunosuppressive therapy. Yamaguchi criteria yield 96.2% sensitivity and 92.1% specificity for AOSD. Although the patient met diagnostic criteria, symptoms were initially attributed to viral illness and reactive arthritis. Diagnostic delay may reflect the acute presentation, atypical age, misleading positive rickettsial serology, and limited disease recognition. The pathogenesis of AOSD remains elusive, though it is generally accepted to be an autoinflammatory disease involving the innate immune system linked to viral triggers. Marked ferritinemia is a key diagnostic clue in distinguishing AOSD from post-viral syndromes.
Tramadol Withdrawal Presenting as Seizure and Encephalopathy
AUTHORS: Kayvon Dehghanian, MD; Lemar Hamilton, MD; Sevak Nersesyans, MD; Ninelle Zargarian, DO; Saira Dar, MD
AFFILIATIONS: Mission Community Hospital Department of Family Medicine
INTRODUCTION: Tramadol is one of the most commonly prescribed analgesics for moderate to severe pain (1,2).It impacts the nervous system through multiple mechanisms, including mu-opioid receptor agonism and inhibition of serotonin and norepinephrine re-uptake (3). Although often regarded as a “safer” opioid, prolonged use of tramadol can lead to dependence and adverse effects, including memory impairment, vomiting, and seizures (4,5). Abrupt discontinuation after long-term use may precipitate withdrawal symptoms such as severe anxiety, insomnia, confusion, and seizures (3,6-8).
METHODS: A 62-year-old woman presented after a new-onset tonic-clonic seizure with tongue biting and urinary incontinence. Family reported recent psychosocial stressors and chronic sleep deprivation. Labs were notable for elevated lactate (17), ammonia (104), and D-dimer (1353). Urine toxicology was positive for benzodiazepines (attributed to prehospital midazolam) and methadone (likely a false positive in the setting of high-dose tramadol use). CT head, MRI brain, and CTA chest were unremarkable. Levetiracetam was initiated for seizure management. EEG demonstrated mild theta–delta slowing consistent with toxic-metabolic encephalopathy without ictal activity. Extensive metabolic and infectious workup was unrevealing. She developed persistent agitation and fluctuating mental status during hospitalization. Further history revealed chronic high-dose tramadol use (300 mg daily), obtained in Mexico, for arthritic pain and headaches, with recent abrupt cessation. Opioid withdrawal was suspected, and buprenorphine was initiated, resulting in rapid clinical improvement prior to discharge.
DISCUSSION: Reported cases of tramadol withdrawal are rare in the literature (6), and our case presents a unique example. This patient was taking 300 mg daily, a relatively high dose compared to the recommended maximum of 400 mg/day (9). The initial seizure may have been related to tramadol’s pro-convulsant effects, possibly via GABA inhibition (10). However, her persistent agitation and encephalopathy following cessation were more consistent with withdrawal. Notably, withdrawal symptoms have been reported at doses as low as 200 mg daily (11). The marked improvement in her agitation and insomnia after initiation of buprenorphine further supports this diagnosis and highlights its potential role as a promising treatment option for tramadol withdrawal (11).
From Anaphylaxis to Tolerance: Managing Heightened Allergic Response to Milk Allergen After Respiratory Virus Infection
AUTHORS: Irene Nguyen, MD (1); Samantha Tope, MD (2), Nicole Nabatkorian, MD (2), Charles Song, MD (2)
AFFILIATIONS: (1) Harbor UCLA Department of Family Medicine, (2) Harbor UCLA Department of Pediatrics
INTRODUCTION: Viral infections, especially human rhinovirus, are associated with asthma exacerbations and theorized to worsen respiratory allergic sensitivity and inflammation. There are less studies documenting viral infections and their potential effects on dietary allergies. In this case, the patient is a 3-year-old female with a history of asthma, allergic rhinitis, and eczema presenting with shortness of breath and diffuse rash after drinking cow’s milk. The patient drank cow’s milk daily prior to this episode but developed an anaphylactic reaction following rhinovirus and enterovirus infection.
METHODS: The patient presented with shortness of breath, wheezing, and diffuse, macular rash after drinking cow’s milk when prior she drank cow’s milk daily without issue. Chest x-ray showed mild peribronchial cuffing and respiratory viral panel was positive for rhinovirus and enterovirus. She was given Duo-nebulizer treatment and an Epipen which resolved her symptoms. Her mother gave her chocolate milk which re-triggered her symptoms and led to admission. During her admission, the patient re-developed wheezing, shortness of breath, and rash twice while NPO and after eating soup with dairy products. In both instances, her symptoms resolved with Epipen administration. Allergy and Immunology (A&I) was consulted for further workup. Relevant lab results include a total IgE 45, milk IgE 2.45, and tryptase 3.5. A&I suspected the patient had a subclinical milk allergy prior to admission, which was worsened by her viral infection. They recommended a 2-day course of IV steroids and inhaled budesonide. Afterwards, the patient was able to tolerate milk and was discharged home.
DISCUSSION: While respiratory viruses are risk factors for asthma exacerbations, it is studied from a respiratory allergen standpoint, not for dietary triggers. There are few studies exploring the theoretical relationship of allergen sensitization and viral infection besides those in mouse or in vitro models. The current theory is that the patient had a subclinical milk allergy and the viral infection increased IgE levels that led to a clinically significant reaction. This theory is seemingly supported by the fact that steroid treatment resolved her reaction to milk. While it is difficult to verify this theory from this case alone, presenting it may help future studies exploring viral infections and their impact on atopic and allergic diseases.
ANCA-Associated Vasculitis in the Setting of Chronic Endemic and Zoonotic Infections: A Diagnostic and Therapeutic Challenge
AUTHORS: Basiru Omisore, MD; Karen Castaneda, MD; Yadira Arguelles, MD; Sheila Toro, MD; Kim Kyung, MD; Syed Hasan, MD; Ebenezer Dadzie, MD; Michael Ozoemena, MD; Ejodakeme Okojie, MD; Kenechukwu Nweke MD
AFFILIATIONS: Rio Bravo Family Medicine Residency Program; Kern Medical Center
INTRODUCTION: Antineutrophil cytoplasmic antibody–associated vasculitis (AAV) can be difficult to diagnose in patients with chronic infections. A 67-year-old cattle worker with chronic coccidioidomycosis presented with progressive neuropathic pain and purpuric rash. Evaluation showed elevated inflammatory markers, positive P-ANCA, and sensorimotor neuropathy. Symptoms improved with corticosteroids. This case highlights the challenge of distinguishing autoimmune vasculitis from infection-related inflammation.
METHODS: A 67-year-old male cattle worker with a history of type 2 diabetes mellitus, hypertension, dyslipidemia, long COVID syndrome, and chronic coccidioidomycosis on fluconazole presented with a 40-day history of progressive bilateral burning foot pain, weakness, and inability to ambulate. He also developed a non-blanching purpuric rash over both lower extremities. Examination revealed distal sensory loss and reduced reflexes. Laboratory studies showed markedly elevated inflammatory markers, hyperferritinemia, high rheumatoid factor, and strongly positive P-ANCA. Renal function was preserved. Extensive infectious evaluation was negative for active infection, though Coxiella burnetii IgG was positive, consistent with prior exposure. Electrophysiologic studies confirmed sensorimotor peripheral neuropathy. Imaging demonstrated chronic fibrotic lung disease without evidence of active infection. Symptoms were refractory to analgesics but improved after initiation of systemic corticosteroids, supporting an immune-mediated vasculitic process.
DISCUSSION: This case highlights the diagnostic complexity of ANCA-associated vasculitis in the setting of chronic infections. The combination of peripheral neuropathy, purpuric rash, elevated inflammatory markers, and positive P-ANCA supports an immune-mediated small-vessel vasculitis. However, chronic coccidioidomycosis and prior Coxiella burnetii exposure complicate interpretation, as infections can mimic vasculitis or induce autoantibody formation. Persistent antigenic stimulation may promote immune dysregulation and trigger autoimmune disease in susceptible individuals. Distinguishing true vasculitis from infection-related inflammation is critical, as immunosuppressive therapy may worsen active infection. In this case, absence of active infection and clinical response to corticosteroids supported
MGUS Presenting with ESBL E. coli Bacteremia, Hypercalcemia, and Electrolyte Imbalances in an Older Adult: A Case Report
AUTHORS: Basiru Omisore, MD; Karen Castaneda, MD; Sheila Toro, MD; Syed Hasan, MD; Kim Kyung, MD; Michael Ozoemena, MD; Ejodakeme Okojie, MD; Kenechukwu Nweke, MD
AFFILIATIONS: Rio Bravo Family Medicine Residency Program; Clinica Sierra Vista; Kern Medical Center
INTRODUCTION: Monoclonal gammopathy of undetermined significance (MGUS) is usually asymptomatic but may be associated with infection risk and metabolic abnormalities. A 67-year-old male presented with sepsis due to ESBL-producing Escherichia coli bacteremia, along with hypercalcemia and electrolyte disturbances. Further evaluation revealed a small clonal plasma cell population consistent with MGUS without evidence of multiple myeloma. The patient improved with antimicrobial therapy and correction of metabolic abnormalities.
METHODS: A 67-year-old male with hypertension, prediabetes, chronic hypokalemia, vitamin D deficiency, and osteoarthritis presented with nausea, vomiting, weakness, and abdominal pain. He had a recent hospitalization for hypokalemia and acute kidney injury that resolved with treatment. On admission, he was mildly tachycardic. Laboratory studies showed leukocytosis, anemia, hypokalemia, hypomagnesemia, hypophosphatemia, and hypercalcemia. Blood and urine cultures grew ESBL-producing Escherichia coli, confirming urinary-source bacteremia. Imaging revealed renal cysts and prostatomegaly without obstruction. He was treated with intravenous meropenem and transitioned to outpatient ertapenem. Hypercalcemia improved with calcitonin and pamidronate. Given persistent anemia and prior monoclonal protein findings, hematologic evaluation revealed a small kappa-restricted clonal plasma cell population consistent with MGUS, without evidence of multiple myeloma. Electrolytes and calcium normalized prior to discharge.
DISCUSSION: This case highlights the interplay between MGUS, infection risk, and metabolic abnormalities in older adults. Although MGUS is often asymptomatic, it may be associated with impaired immune function, increasing susceptibility to severe infections such as ESBL-producing bacteremia. Hypercalcemia in this context raises concern for progression to multiple myeloma, but alternative causes such as infection and dehydration must be considered. Careful evaluation is essential to avoid misdiagnosis and unnecessary treatment. In this patient, normalization of calcium with supportive care and absence of myeloma-defining features supported MGUS rather than malignancy. Multidisciplinary evaluation and close follow-up are critical to guide management and monitor for progression.
From Urinary Tract Infection to Spinal Sepsis: Escherichia coli–Associated Psoas Abscess and Vertebral Osteomyelitis in an Elderly Patient with Diabetes Mellitus
AUTHORS: Basiru Omisore MD; Karen Castaneda MD; Sheila Toro MD; Syed Hasan MD; Kim Kyung MD; Michael Ozoemena MD; Ejodakeme Okojie MD; Kenechukwu Nweke MD
AFFILIATIONS: Rio Bravo Family Medicine Residency Program; Clinica Sierra Vista; kern Medical Center
INTRODUCTION: Vertebral osteomyelitis with epidural and psoas abscess is a serious complication of untreated infection. A 72-year-old diabetic woman presented with severe back pain after recent urinary tract infection. Imaging revealed T12–L2 discitis, a large psoas abscess, and a small epidural abscess. Cultures confirmed Escherichia coli from a urinary source. She improved with drainage and targeted antibiotics. This case highlights the need for early recognition of atypical pain and appropriate therapy.
METHODS: A 72-year-old woman with poorly controlled diabetes presented with progressive left flank and severe back pain following recent treatment for urinary tract infection. She had been discharged on empiric antibiotics prior to culture results. Despite therapy, her pain worsened and limited mobility. On admission, she was afebrile but had leukocytosis and elevated inflammatory markers. Imaging revealed T12–L2 discitis–osteomyelitis, a large left psoas abscess, and a small epidural abscess without neurologic compromise. Interventional radiology performed drainage of the psoas abscess. Cultures from urine, abscess fluid, and bone biopsy grew Escherichia coli, confirming a common source. Blood cultures were negative. She was treated with intravenous ceftriaxone and managed conservatively for the epidural abscess. Clinical status improved with reduced pain and declining inflammatory markers. She was discharged on prolonged intravenous antibiotics with close follow-up.
DISCUSSION: This case demonstrates progression of urinary tract infection to spinal infection in a high-risk diabetic patient. Poor glycemic control impairs immune function, increasing susceptibility to deep tissue spread. Persistent or severe back pain beyond typical urinary infection should prompt early imaging to evaluate for complications such as osteomyelitis or abscess. Suboptimal initial antibiotic therapy may contribute to disease progression. Targeted antimicrobial treatment and timely source control are critical. Select epidural abscesses without neurologic deficits can be managed nonoperatively with close monitoring. Multidisciplinary care is essential to optimize outcomes.
Severe, Progressive Infantile Seborrheic Dermatitis: Recognizing Atopic Dermatitis Overlap and Management Challenges
AUTHORS: Shivam Patel OMS-III, Moira Williams OMS-III, Pooja Patel MS-1, Samhrutha Reddy Sripathi MD, Sudha Ranganathan MD
AFFILIATIONS: Rio Bravo Family Medicine/Clinica Sierra Vista/Kern
INTRODUCTION: Infantile seborrheic dermatitis is generally a benign and self-limited chronic inflammatory skin condition, however more severe presentations with extensive erythema, scaling, and crusting suggests underlying skin barrier dysfunction with atopic dermatitis (AD) complicating diagnosis and traditional management. We hypothesize that impaired skin barrier function associated with AD characterized by increased transepidermal water loss and enhanced susceptibility to microbial colonization, facilitated an exaggerated inflammatory response to Malassezia, contributing to the severity of this case.
METHODS: At 2 months, the patient presented with mild cradle cap and small areas of facial dryness, consistent with infantile seborrheic dermatitis and xerosis. He was treated with topical ketoconazole. Over the next 16 days, at 3 months of age, the dermatitis progressed, involving the face, cheeks, and auricles, with yellow, flaky, crusted plaques and excoriations, especially on the cheeks and temporal scalp. The mother reported significant pruritus with frequent scratching and sleep disruption, worse at night. Topical mupirocin was started for excoriations. Cultures showed gram-positive clusters, but no systemic symptoms; given expected presence of Staphylococcus aureus as normal flora, no further treatment was pursued. Growth and development were appropriate, with no systemic concerns. 3 days later, flaking improved and lesions were healing, but diffuse erythema and inflammation persisted raising concern for underlying atopic dermatitis. Treatment was escalated to triamcinolone 0.025% (body) and desonide 0.05% (head/neck) twice daily for 3 weeks. Pediatric dermatology diagnosis is pending.
DISCUSSION: A key feature in this case is the potential underlying atopic dermatitis complication ISD management. Together, these factors may create a cycle of inflammation, barrier disruption, and disease propagation, distinguishing more severe presentations, which providers should recognize. While disease severity warrants the use of topical corticosteroids, clinicians should remain mindful of associated risks in infants. Prompt referral to a pediatric dermatologist allows for consideration of steroid-sparing therapies and further evaluation of underlying dermatologic conditions. Beyond initial resolution, referral to an allergist for assessment of food allergies given association in up to 33% in those with AD should be considered as workup could prevent serious complications in childhood.
A Case of Recurrent Pulmonary Aneurysms and Massive Hemoptysis
AUTHORS: Kevin Tan, Kaycee Ching, Natalie Mourra, Bruno Lewin
AFFILIATIONS: Family Medicine Residency Program at Kaiser Los Angeles Medical Center
INTRODUCTION: Hughes-Stovin syndrome (HSS) is a rare systemic vasculitis defined by arteriovenous thromboses accompanied by pulmonary or bronchial aneurysms. Its rarity — with fewer than 50 reported cases in the literature — means most clinical knowledge derives from case reports alone. Early recognition is critical given the high mortality associated with massive hemoptysis. We present a 24 yo female with Crohn's disease, recurrent thromboembolic disease refractory to anticoagulation, and right atrial mural thrombus who was admitted with recurrent hemoptysis, and ultimately diagnosed with HHS.
METHODS: A 24-year-old female was admitted for recurrent hemoptysis after a decade of complex multisystem illness. Prior workup identified Crohn’s disease and chronic inferior vena cava thrombosis, treated with enoxaparin, adalimumab, and methotrexate. Imaging showed recurrent pleural and pericardial effusions. Echocardiography revealed severe tricuspid regurgitation with right-sided dilation, and cardiac MRI demonstrated a band-like mass along the right interventricular septum. She later developed pulmonary embolism and cardiogenic shock; transesophageal echocardiography showed worsening right ventricular dysfunction with a new right atrial mass, which improved after thrombectomy. Rheumatologic workup was unrevealing. A right lower lobe pulmonary pseudoaneurysm required lobectomy, with no vasculitis on pathology. On this admission, imaging revealed a left interlobar artery aneurysm and pulmonary embolism; surgery was deferred given the location. Karius testing was negative. Hemoptysis resolved, but she later suffered cardiac arrest and died.
DISCUSSION: HSS is exceedingly rare, with evidence limited to case reports. In this case, diagnostic anchoring and unfamiliarity contributed to a decade-long delay in diagnosis. The patient’s atypical presentation and limited female cases likely compounded this delay. Although Interventional Radiology raised concern for HSS, this was not pursued due to prolonged admission and team turnover. Upon transition to a new primary team, deidentified clinical information was entered into a large language model, which identified HSS as the leading diagnosis and prompted renewed evaluation - leading to the diagnosis. This case highlights the diagnostic pitfalls in recognizing rare diseases and the potential role of LLMs as adjuncts in expanding differentials, particularly when rare diagnoses may be overlooked.
Latrogenic Calciphylaxis and Its Subsequent Successful Management
AUTHORS: Melody Wang, MD; Stefanie Wu, MD
AFFILIATIONS: Department of Family Medicine, Kaiser Los Angeles Medical Center
INTRODUCTION: Calciphylaxis, also known as calcemic uremic arteriolopathy, is a very rare and serious disease characterized by the calcification of the small and medium arteries that leads to subsequent tissue ischemia and infarction. The pathogenesis is unknown. It occurs most commonly in patients with end-stage kidney disease, though other common factors to consider are warfarin and prolonged corticosteroid use. Affected patients suffer from painful skin lesions, and is otherwise a highly fatal condition with one-year-mortality being greater than fifty percent due to sepsis.
METHODS: The patient is an 80 year-old-female with hyperlipidemia, hypertension, and extensive bilateral chronic venous stasis ulcers. She initially presented for follow-up in the vascular surgery clinic for wound checks and was found to have significantly worsening right lower extremity wounds tracking proximally towards her knee. She was subsequently transferred to the emergency room, where she had stable vitals with a normal creatinine, mild leukocytosis, and was started on intravenous antibiotics. The inpatient vascular team performed another debridement and ultimately decided to take a biopsy of the selected area due the severity of the wounds. After extensive review with pathology and dermatology-pathology, the biopsy yielded diffuse ulceration and dermal/subcutaneous necrosis with vascular thrombosis and calcifications, favoring calciphylaxis. With the guidance of dermatology, the patient was started on sodium thiosulfate and discharged with routine follow-up with vascular surgery. She continues to improve, though it is still uncertain what initially may have caused her calciphylaxis.
DISCUSSION: In the context of severe and aggressive wounds, it is imperative to keep an open differential of the underlying cause, and a biopsy of the area may be indicated. Though exceedingly rare, calciphylaxis can still occur in patients without any contributing renal history. If confirmed, a multidisciplinary approach is needed for appropriate patient management. Sodium thiosulfate is the primary treatment. Patients should start with a test dose of 12.5g daily over 30 minutes through a PICC line with monitoring for hypotension. If tolerated, the dose can be advanced 48 hours later to 25g over 60 minutes after, and should be continued three times per week until symptoms improve. The patient then should follow up with a specialist to determine whether to stop or continue these treatments.
Lectern Session 2 (3:05 – 3:50PM)
Structured Low-Dose Aspirin Protocol Improves Screening, Prescribing and Maternal Outcomes: A quality improvement–informed quasi experimental pre–post study
AUTHORS: Nariman Almnini, MD; Samhrutha Sripathi, MD; Yvette Singh, MD; Verna Marquez, MD
AFFILIATIONS: Rio Bravo Family Medicine Residency Program, Bakersfield, CA, USA
INTRODUCTION: Preeclampsia is a leading cause of maternal and perinatal morbidity and mortality. Evidence suggests abnormal placentation involving angiogenic imbalance, endothelial dysfunction, inflammation, and thrombosis as key mechanisms. Low dose aspirin (LDA), through cyclooxygenase1 inhibition, reduces platelet aggregation and inflammation. Randomized trials and meta-analyses demonstrate that early LDA initiation reduces the risk of preterm preeclampsia; however, structured LDA screening and prescribing protocols remain limited in federally qualified health centers.
METHODS: We conducted a quasi-experimental pre–post cohort study comparing pregnancy outcomes before and after implementation of a structured low dose aspirin (LDA) screening and prescribing protocol at a federally qualified health center. Pregnant patients receiving care prior to protocol implementation served as historical controls, while those receiving care after implementation were prospectively screened according to standardized criteria. Primary outcomes included preeclampsia, gestational hypertension (GHTN), and preterm birth. Postimplementation adherence to LDA was assessed.
RESULTS: Ninety-two patients were included in the pre-implementation cohort; 51 were prescribed LDA, with 9.8% developing preeclampsia and 4.3% experiencing preterm birth. Adherence to LDA was not available for this cohort. Postimplementation, 156 patients were screened; 7 were excluded, and 120 met criteria for LDA, of whom 117 were prescribed aspirin. Among those prescribed LDA, 84 were adherent, and 33 were noncompliant. Preeclampsia incidence was significantly lower among adherent patients compared with noncompliant patients (3.6% vs 15.2%; p=0.0329). Rates of GHTN and preterm birth did not differ significantly between groups (p=0.2016 and p=1.0, respectively).
CONCLUSIONS: Implementation of a structured LDA screening and prescribing protocol in a federally qualified health center was feasible and associated with improved adherence and a significant reduction in preeclampsia among compliant patients. No significant differences were observed in rates of gestational hypertension or preterm birth. These findings support structured LDA protocols as an effective quality improvement strategy to reduce preeclampsia risk in high risk, safety net populations, with larger studies needed to assess effects on additional maternal outcomes.
Disparities in Telehealth Use Among Adults with Diabetes in California
AUTHORS: David Bales, MD (1), Beza Mengistu (2), Ann M. Hernandez, MD, MPH, MS (1,2)
AFFILIATIONS: (1) Department of Family Medicine at UCLA, (2) David Geffen School of Medicine at UCLA
INTRODUCTION: Telehealth is an undeniably valuable resource for enhancing care and improving health outcomes in patients with diabetes. Research on the national level has demonstrated that telehealth appointments, as a complement to in-person visits, can significantly improve patients’ glycemic control. However, telehealth is not without its barriers to patient access and effective use that vary based on a multitude of different patient-specific factors. This project evaluates the 2024 California Health Interview Survey (CHIS) to identify demographic patterns of telehealth use in patients with a self-reported diagnosis of diabetes.
METHODS: We conducted a cross-sectional analysis of the 2024 California Health Interview Survey (CHIS) public use file, a population-based survey of noninstitutionalized adults in California. Adults (≥18 years) with self-reported diabetes were included. The primary outcome was any telehealth use in the past 12 months. We used descriptive statistics to estimate the prevalence of telehealth use and to characterize the study population. Bivariate analyses examined differences in telehealth use across sociodemographic characteristics, including age, sex, race/ethnicity, insurance, and income. Survey weights were applied to account for the complex sampling design and generate population-representative estimates.
RESULTS: Hispanic and Asian patients were less likely to have seen a provider via telehealth when compared to White or African American patients (p < .001). Additionally, male patients were less likely to have utilized telehealth than female patients (p < .001). Patients who reported their education level as “none to high school diploma” were less likely to have used telehealth (p < .001), though there was no difference when patients were stratified based on employment status and income relative to the federal poverty level. Patients without insurance or usual sources of healthcare were less likely to have experienced telehealth (p < .001), while patients with comorbid conditions such as hypertension or heart disease were more likely to have done so (p < .001 and p = .01, respectively).
CONCLUSIONS: Disparities in telehealth use by insurance status, usual source of care, race/ethnicity, and education suggest inequitable access among adults with diabetes. However, greater use among those with comorbidities suggests telehealth is reaching higher-need patients already connected to care. These findings reinforce the importance of targeted outreach to specific populations and systemic efforts to improve infrastructure to provide access to telehealth resources with the goal of optimizing clinical management in patients with diabetes.
A Gratitude-Based Intervention Improves Professional Fulfillment Among Family Medicine Residents
AUTHORS: Kiana Panbechi, DO, and Cindy Yang, MD
AFFILIATIONS: Dignity Health Northridge Family Medicine Residency Program, Northridge, CA
INTRODUCTION: Resident physicians consistently report high rates of burnout and stress throughout training. Wellness, however, is more than the absence of burnout and includes protective factors such as professional fulfillment and gratitude, which are associated with meaning, satisfaction, resilience, and engagement in clinical work. Gratitude-based practices have been shown to enhance well-being and team connectedness in healthcare workers. This study evaluated whether a brief, peer-recognition gratitude intervention could improve professional fulfillment and gratitude among family medicine residents.
METHODS: This prospective single-arm pre-post pilot study included approximately 23 family medicine residents at a single residency program. Participants completed baseline surveys assessing professional fulfillment (Professional Fulfillment Index, 6 items) and gratitude (2 single-item measures). The 4-week intervention included a 30-minute workshop on positive psychology and a peer-recognition “kudos card” practice integrated into weekly lectures. Post-intervention surveys repeated outcome measures and assessed feasibility. Paired t-tests were used to compare pre- and post-intervention scores, with effect sizes calculated using Cohen’s dz. Correlation between changes in gratitude and fulfillment was assessed.
RESULTS: Twenty residents completed paired surveys. Professional fulfillment increased from 2.75 ± 0.40 to 3.11 ± 0.42 (Δ = +0.36, p = 0.033, dz = 0.53), representing a statistically significant improvement. Gratitude outcomes were mixed: “I have so much in life to be thankful for” increased significantly from 5.32 ± 1.20 to 6.32 ± 0.89 (Δ = +1.00, p = 0.048, dz = 0.49), while “Overall, I am a grateful person” increased from 5.28 ± 1.27 to 5.83 ± 1.05 (Δ = +0.56, p = 0.21, dz = 0.30), which was not statistically significant. Changes in gratitude were strongly and significantly correlated with changes in professional fulfillment (r = 0.66, p = 0.002).
CONCLUSIONS: A brief, low-cost gratitude-based intervention was associated with a statistically significant improvement in professional fulfillment and a moderate increase in gratitude among family medicine residents. The strong correlation between changes in gratitude and fulfillment suggests a potential mechanism linking positive psychology practices to enhancing physician wellness. These findings support the feasibility, acceptability, and potential impact of scalable, peer-based interventions to promote resilience and well-being in residency training.
Addressing Health Disparities: A Pathway Program to Support Pre-Health Underrepresented Minorities in the Health Professions
AUTHORS: Mahuya Barua, Carina Franco, Ariana Rodriguez, Juan Carlos Sanabria, Rosa Vasquez, Elias Geronimo de Leon, Catalina Bayardo, Gilberto Granados, Jyoti Puvvula
AFFILIATIONS: Harbor-UCLA Department of Family Medicine
INTRODUCTION: The ethnic diversity of the United States is increasing; however, African American, Latinx, and Native American remain significantly underrepresented in medicine (URiM). Many URiM students are first-generation college attendees and lack access to mentorship, guidance, and resources needed to pursue health careers.
The Summer Urban Health Fellowship (SUHF) is a pathway program designed to support URiM students. The program provides structured mentorship, academic enrichment, including clinical shadowing, application preparation, and individualized coaching to strengthen participants’ readiness for health profession school applications. .
METHODS: We sought to assess the impact of SUHF among our undergradute students and those in their gap years. We analyzed SUHF evaluation data completed by pre-health professions participants for the past three years from 2023 through 2025. We looked to see which of the various components of the program including pre-health professions application workshops, such as mock-interviews, personal statement writing, clinical shadowing, community engagement, and individualized coaching among others were perceived as most beneficial by the participants.
RESULTS: Of the 59 pre-health professions participants from 2023-2025, over 75% identified as URiM (10% African American, 66% Latinx), 54% were first-generation college students, and more than 60% came from non–English-speaking households, most commonly Spanish-speaking. Participants reported that skill-building workshops, including mock interviews and personal statement development, significantly improved their confidence in the application process. Experiential learning, such as shadowing family physicians in underserved settings, including care for migrant and unhoused populations and community engagement were also rated as highly influential in shaping interest in health careers. Notably, 80% of participants indicated an increased likelihood of practicing in medically underserved areas.
CONCLUSIONS: Pathway programs that provide mentorship, skill-building, and exposure to underserved communities can enhance URiM students’ confidence and preparedness for health professions training while fostering commitment to serving marginalized populations.
Thank You
Acknowledgements
The Multi-Campus Research Committee expresses deep appreciation to Dr. Gerardo Moreno and the UCLA Department of Family Medicine for their continued financial support of the Multi-Campus Research Forum.
We are especially grateful to the HRSA-funded UCLA DGSOM Center of Excellence (UCLA COE) for its financial support of this year’s Research Forum.

A huge thank-you to Damilola Jolayemi, Uyen Kao, and Enrique Sanchez (from UCLA CHIPTS), and Felicia Winningham and Valencia Moody (from UCLA Family Medicine), for their invaluable assistance with event coordination.
Last, but certainly not least, the Committee is extremely grateful for the administrative direction of Laura W. Sheehan, who has been running this event since she joined UCLA Family Medicine over 13 years ago.
Raffle
We encourage all attendees to please stay for the entirety of this year's event. We will be raffling Amazon gift cards for three lucky attendees at the very end of Research Day. If you are able to stay until the end of today's event (4pm), please be sure to enter the raffle at the Check-In desk to enter your name into the raffle. You must be present to win!