Sleeve Weight Regain
Find Your Care
Our bariatric surgeons use a range of treatments to help you reach weight loss goals and optimize your health. To learn more, call 310-206-0367.
Weight regain after gastric sleeve
Sleeve gastrectomy (SG) is the most popular bariatric procedure in the US and worldwide. Small amounts of weight regain 1-2 years after surgery are normal and expected.
A subset of patients can regain most lost weight back in a few years after sleeve gastrectomy. Significant weight regain can lead to the recurrence of obesity-related comorbidities and decreased quality of life. While most patients can lose more than 50% of the excess weight one year after sleeve gastrectomy, some patients may have inadequate loss.
Causes of weight regain after sleeve gastrectomy
Potential causes of weight regain or inadequate weight loss include large remnant stomach (pouch) size, gradual increase of remnant stomach volume, increased sweet consumption and portion size, emotional eating, and binge eating.
Treatment options
Significant weight regain after bariatric surgery presents one of the biggest challenges for patients. Dietary and lifestyle modification, weight loss medications and revision surgery are the main treatment options.
Dietary and lifestyle modification
Small and frequent meals (eating 3-5 times a day), healthy food and exercise are the keys for long-term success.
We encourage all our patients to keep a food journal to help them to document the nutrition intake and identify any triggers. The goal is to consume about 80-100 grams of protein per day and eat plenty of fiber rich fruits and vegetables. Avoid foods with high fat, sugar and salt content. Ensure adequate hydration (at least 64 fl oz of water daily) and sleep (7-8 hours daily) will help prevent weight regain. Avoid late night eating, fast and convenience foods. Practice meal planning and plan grocery shopping ahead of time to avoid purchasing trigger food items. Choose healthier items such as lean proteins (chicken, turkey, fish), non-starchy vegetables, complex carbohydrates (whole grains), fruits and low sugar/ low-fat options.
Even with a much smaller stomach, loss of control can still happen to some patients, thus developing sustainable lifestyle changes will be key to long-term success.
Using food timers can help avoid mindless eating or grazing throughout the day by promoting eating at designated times.
A good exercise regimen is very important for long-term weight management. The ideal goal is to have 150 minutes of cardio and 2-3 days of strength training per week. Common cardio exercises include dancing, running, swimming, brisk walking, aerobics, kickboxing, skiing, surfing, and bike riding. Common strengthening activities include using free weights, resistance bands and weight machines.
Weight loss medications
In addition to dietary and lifestyle modification, the use of weight loss medications should be considered for patients with weight regain after sleeve gastrectomy. The commonly used medications include Orlistat, Phentermine/Topiramate, Phentermine, Liraglutide and Semaglutide.
Starting weight loss medications after bariatric surgery should be an individualized decision. We encourage all patients with weight regain issues to discuss this option with their bariatric surgeon/bariatrician. Semaglutide (Ozempic or Wegovy) has been shown to have robust weight loss for obese patients. Even though it has not yet been specifically studied in the post-bariatric surgery population, it is still a very reasonable option for patients with weight regain or inadequate weight loss.
Revision Bariatric Surgery
For weight regain patients who do not respond to conservative medical treatment, revision surgery can be considered.
The choices of revision procedures for weight regain or inadequate weight loss after sleeve gastrectomy include Roux-en-Y gastric bypass (RYGB), one-anastomosis gastric bypass (OAGB), re-sleeve gastrectomy (re-SG), endoscopic gastropasty (ESG), single-anastomosis duodeno-ileal bypass (SADI), and duodenal switch (DS).
Among these revision procedures, conversion to RYGB and OAGB are the two most widely performed and well recognized procedures for weight regain/inadequate weight loss after sleeve gastrectomy.
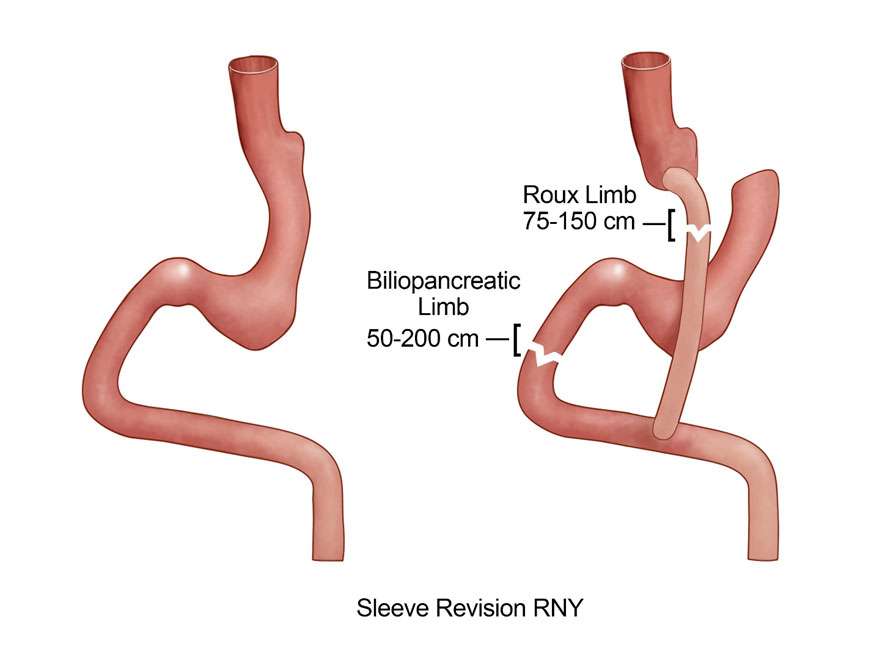
Conversion to Roux-en-Y Gastric Bypass
During the conversion surgery, the stomach is divided, and a small pouch is created, then the small bowel is connected to this small pouch. Finally, the Roux-limb of the small bowel is connected to the biliopancreatic limb of the small bowel.
If the indication for conversion is due to weight regain/inadequate weight loss, patients can expect to lose 30-70% of the excess weight. With the weight loss, many patients have resolution of obesity related comorbidities. The standard RYGB has a biliopancreatic limb of 50 cm. For RYGB with longer biliopancreatic limb (100-200 cm), recent studies suggest that the weight loss is better. There is no nutrient absorption in the biliopancreatic limb. For patients with weight regain after sleeve gastrectomy who need to have conversion surgery, a long biliopancreatic limb can be considered to maximize the weight loss.
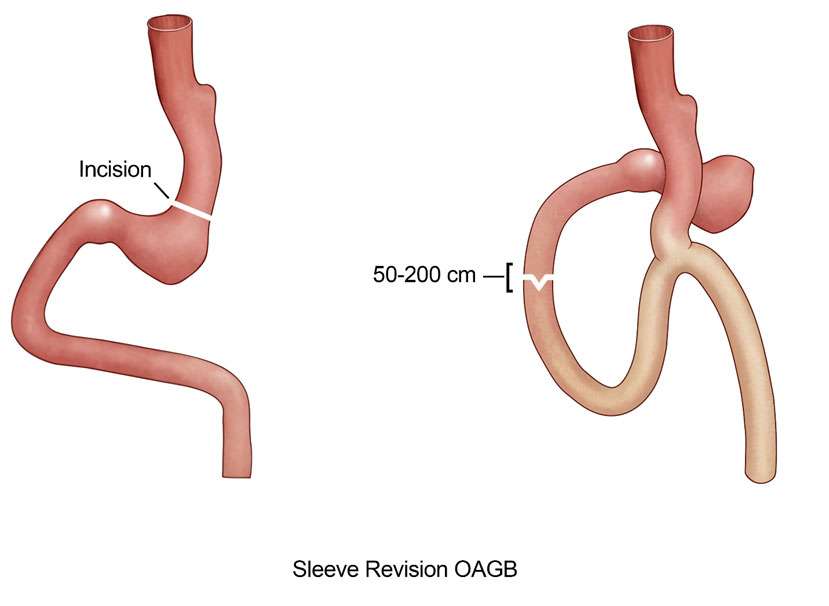
Conversion to One-Anastomosis Gastric Bypass
Conversion of sleeve gastrectomy to OAGB is performed by creating a long gastric pouch (much longer than the standard Roux-en-Y gastric bypass) first. Then the small bowel is connected to this long gastric pouch. The biliopancreatic limb (150-200 cm) in OAGB is longer than the standard Roux-en-Y gastric bypass surgery (50 cm). Patients can expected to lose 50-85% of the excess weight.
Both conversion to RYGB and OAGB are good options for patients with weight regain or inadequate weight loss after sleeve gastrectomy. Quite a few studies have shown that the weight loss of conversion to OAGB is slightly better than conversion to RYGB, likely due to the longer biliopancreatic limb.
Contact Us
To schedule a consultation with UCLA Bariatric Surgery in Los Angeles, California, call us at 310-206-0367 or fill out our online form
*Weight loss results can vary depending on the individual. There is no guarantee of specific results. Read full disclaimer.