Breast Augmentation
Find your care
Our team is made up of experts and leaders in the art and science of plastic surgery. To learn more about our services, call 310-825-5510.
Thinking about a breast augmentation?
You're not alone. According to the American Society of Plastic Surgeons (ASPS), last year more than 290,000 American women chose to surgically enhance the size, shape, and aesthetic appearance of their breasts. Odds are you know some who has either had their breasts augmented or has at least asked many of the same questions that you are likely asking. While the information that follows is meant to provide you with a broad overview and some basic answers to many of those questions, it is no substitute for a consultation with one of our cosmetic surgeons.
Clinic hours:
8:00 AM to 5:00 PM - Monday through Friday.
The Procedure
There are a number of different ways a breast augmentation can be performed. Your surgeon will advise you on the technique best suited to your desired outcome. Breast implants may be placed either subpectorally (under the pectoralis muscles at the base of the breast) or subglandularly (under the breast gland only and on top of the pectoralis major muscle).
Subpectoral
The principle advantage of subpectoral placement is that it statistically lowers the risk of capsular contracture. (Capsular contracture is part of the body's natural immune response to foreign objects. The actual mechanism that causes this is largely unknown, but essentially, the implant pocket begins to tighten around the implant and squeeze it to the point where the implant may shift position within the breast.) The subpectoral placement also has the advantage of allowing better overall soft tissue coverage and a more natural transition in the upper poles of the breast. And if a mastopexy (breast lift) becomes necessary in the future, the subpectoral placement increases the vascular viability of the nipple / areola region and decreases the likelihood of post-mastopexy complications.
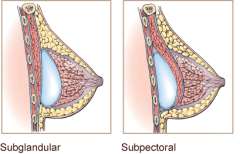
Subglanular
Subglandular placement of the implants can achieve better (more natural) aesthetic results in cases of breast ptosis. Subglandular implantation is also less painful and patients enjoy a faster overall recovery period.
The Incision
The placement of the implant, the depth of the surgical pocket created to hold the implant, and the type of incision used will all have an effect on the final aesthetic appearance of the augmented breast.
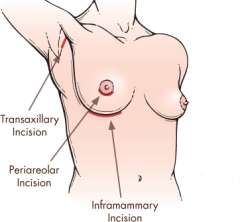
Inframmary
The most common incision used is an inframammary approach, which places the incision transversely at the level of the inframammary fold (along the base of the breast). The incision offers a well-concealed scar underneath the fold of the breast, with no visible scarring on the breast itself.
Periareolar
The periareolar approach places the incision at the junction of the areola and normal non-pigmented breast skin. The advantage to this approach is that it conceals the scar along the border of the areola, and there is no visible scarring on the breast itself. The disadvantage to this approach is that it results in a higher incidence of diminished nipple sensitivity, and there is also the potential that a periareolar incision will damage the ductal structures of the breast, inhibiting the ability to breastfeed in the future. Another disadvantage to this approach is that it limits the ability to revise the surgery to improve the aesthetic results, and attempted revisions can result in a tethering or inversion of the resulting scar when the periareolar incision is repeatedly reopened.
Transaxillary
The transaxillary approach allows placement of the implant through the axilla (armpit), with no scars whatsoever on the breast itself. Surgical visualization, however, is poor and this approach increases the likely need for surgical revision to correct implant malposition. Surgical revisions via transaxillary incision are extremely difficult to perform and often require a secondary incision resulting in surgical scarring of the breast.
Transumbilical
The transumbilical approach is the least frequently used surgical approach. The scar is limited to the peri-umbilical region (navel). The disadvantage to this approach is that it only allows for the use of saline implants. Revisions cannot be performed using this approach, and a secondary incision, with resulting surgical scarring, would be necessary to correct any malposition of the breast implant. Nevertheless, for certain patients and experienced surgeons, it is a viable option.
Choosing the Right Implant
Implants come in a variety of sizes and styles. Slicone, saline, and gel implants have an elastomer shell (a type of plastic designed to stretch rather than rupture that will not break down in the naturally occurring heat of the human body). As their names imply, silicone implants are filled with a liquid silicone gel, while saline implants are filled with saline (salt water).
However, rather than worrying about what type of implant, it's better to focus on the aesthetic result you want to achieve. Your desired look is more than just a matter of size. Size is a simple measure of the volume of your new breasts. Your augmentation will enhance the size, shape, proportion, and feel of your breasts.
You can achieve a teardrop or round shaped result based on a number of different factors, including your existing breast type and the dimensions of the breast implant used. A teardrop shaped result has a gradual, sloping profile from the top of your chest to your nipple. Women who want a teardrop shaped result often want breast implants to restore the youthful appearance of their breast.
A round shaped result has a more obvious profile with a more prominent look, a higher ridge atop the chest, steeper cleavage and an extended side profile. Women who want a round shaped result often have an emphasis of achieving a larger cup size.
Once you share your goals and discuss your desired outcome with your surgeon, he or she will help you select the appropriate implant.
Know the Risks
Unlike most other cosmetic procedures, which typically only carry a short-term post-operative risk for complication, breast augmentation is unique in that the risk for complications extends over the life of the implant. One in five women will require some form of re-operation within the first three years of augmentation. The most common reason for re-operation is to improve the aesthetic result: the implant may be poorly positioned, giving the breast a less-than-desirable contour, or the implant selected may have been the wrong size--either too large or too small--for the desired post-operative shape of the breast.
Complications can include:
- Hematoma
- Infection
- Changes in nipple sensation
- Capsular contracture
- Implant rupture
- Implant malposition (immediately post-operative)
- Impaired mammographic visualization.