Aortic Valve Disorders
Find Your Care
Interventional cardiology teams provide care in multiple locations. To learn more about our services, call 310-825-9011.
UCLA Health ranks as one of the top hospitals in the nation according to U.S. News & World Report. Our cardiology and heart surgery program consistently ranks among the top in the nation and has been recognized on the American Heart Association (AHA) Target Aortic Stenosis (AS) Honor Roll in 2024 and 2025 for excellence in aortic stenosis care.

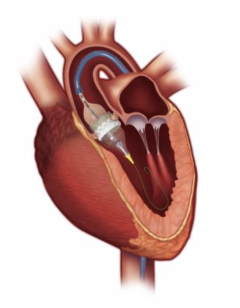
This animation shows how the Edwards SAPIEN 3 TAVR valve is implanted using a minimally invasive transfemoral approach.
What Is Aortic Valve Stenosis?
Aortic valve stenosis is a heart condition where the valve that controls blood flow from the heart does not open fully. This can cause chest pain or tightness, tiredness, shortness of breath during activity, and sometimes dizziness or fainting.
Surgery to replace the valve is a common and effective treatment. However, surgery is not an option for all patients. For patients who can’t undergo surgery, a new valve can be inserted through a small puncture in the groin or another access point, avoiding the need for open-heart surgery.
TAVR Procedure for Aortic Valve Disorders
The U.S. Food and Drug Administration (FDA) approved the transcatheter aortic valve replacement (TAVR) in 2011 as an alternative to surgery for patients with aortic valve stenosis. In 2016, approval was extended to patients at moderate risk for surgery. In August 2019, it was approved for low-risk patients. Today, patients with severe AS who have symptoms should be evaluated by a heart team of cardiologists, cardiomyopathy specialists and cardiac surgeons and can be considered for TAVR.
The TAVR procedure involves placing a long, flexible tube (catheter) with a new valve in an artery and guiding it to the heart. This new valve is then deployed inside of the native, diseased valve.
Because TAVR surgery uses minimally invasive techniques, patients usually recover faster and experience improved blood flow right after the procedure, compared with traditional open-heart valve replacement. While the procedure is less invasive than open-heart surgery, it should be taken seriously in terms of preparation and recovery.
Our Multidisciplinary Team Approach
The heart team at UCLA Health includes interventional cardiologists, noninvasive cardiologists, cardiothoracic surgeons and anesthesiologists. UCLA Health has been performing TAVR procedures since 2012 and has achieved excellent outcomes. Since 2015, most patients have had TAVR with moderate sedation instead of general anesthesia, which helps improve the safety of the procedure. Using the newest generation devices, most patients are treated through the transfemoral approach, but the team also has experience with alternative approaches, including transcarotid, transaxillary and transapical, when needed. If you have questions about any of these approaches, please ask your doctor.
UCLA Health has led the nation in TAVR outcomes and has hosted conferences and seminars to teach best practices to visiting teams from across the U.S. and around the world.
Listen to Dr. Aksoy talk about Aortic Stenosis and its treatment
What to Expect
Once patients are referred for evaluation, appointments are scheduled to meet with both the cardiologist and surgeon on the same day at UCLA Health. If not already done, a CT scan to check access and valve size is completed during these appointments. After reviewing imaging and consultations, the heart team recommends the best course of action. If the TAVR procedure is recommended, the team may also check for the need for a coronary angiogram and request dental clearance, since dental infections are a common source of heart valve infections. The procedure date is then set. Many patients are discharged one to two days after TAVR and expected to fully recover within one to two weeks.
On the day of TAVR surgery, patients check in at the hospital. After preparation, the procedure is performed. Patients are monitored for valve function and medications are adjusted as needed. Once stable, follow-up appointments are arranged at one week, one month and one year, including echocardiograms.
UCLA Health is currently evaluating patients who may need TAVR. For more information or to schedule an evaluation, please call the number below.
Contact Information
UCLA TAVR Coordinators:
Jeanne Huchting, NP
Maria Gultom, NP
Jill Polina-Belcher, RN
Phone: 310-825-9011
Fax: 310-825-3433
Email: [email protected]
Locations
UCLA Health performs the TAVR procedure at Ronald Reagan UCLA Medical Center and UCLA West Valley Medical Center.

Ronald Reagan UCLA Medical Center










