Acromegaly
Find your care
We treat pituitary tumors using the latest innovations in minimally invasive procedures. To connect with an expert in the pituitary tumor program, call 310-825-5111.
Acromegaly is condition that is nearly always caused by a pituitary adenoma, a tumor of the pituitary gland. The term acromegaly literally means enlarged extremities; acro means extremity and megaly means enlargement of.
Acromegaly Treatment in Southern California
Our comprehensive approach to diagnosis and treatment of pituitary conditions, including acromegaly, sets the UCLA Pituitary Tumor Program apart. Our physicians treat a high volume of patients every year and perform over 100 pituitary surgeries a year, making us one of the top programs in the United States.

Use these links to explore more about acromegaly:
Acromegaly: Physiology
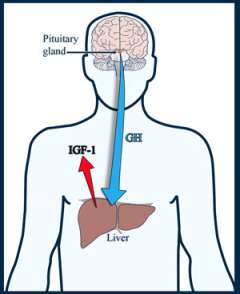
The normal pituitary gland secretes growth hormone (GH):
- In childhood, GH is important for proper development and growth of the body.
- In adults, GH maintains healthy bone and muscle function.
GH has direct effects on the body, such as on muscle growth. It also acts on specialized gland cells in the liver:
- This leads to the release of a hormone called insulin-like growth factor (IGF-1, or somatomedin-C) into the blood stream.
- IGF-1 blood levels are much steadier compared to GH, which changes dramatically throughout the day.
- IGF-1 affects many organs of the body, particularly bone and cartilage.
A pituitary tumor that secretes an excessive amount of GH causes changes in the body that lead to disfigurement. If the disfigurement severely affects the internal organs, it could lead to death.
While acromegaly is nearly always caused by an adenoma, there are rare cases when it occurs due to excess growth hormone secretion outside the pituitary. These tumors most commonly occur:
- In the lung (bronchial carcinoid)
- In the pancreas (pancreatic carcinoid)
Acromegaly typically presents in adulthood. Because the physical changes occur so slowly, it can take an average of seven to eight years before the condition is diagnosed. If a pituitary tumor produces an excessive amount of GH in childhood, gigantism occurs.
Acromegaly: Symptoms

Acromegaly: Symptoms Related to Excess GH
- Abnormal enlargement of the hands and feet
- Rings no longer fitting
- Widening of the distal fingers and toes, sometimes referred to as "paddle" toes
- Hands feeling soft like bread dough
- Enlargement of the feet requiring a larger shoe size
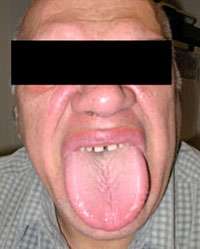
- Changes in facial features, sometimes quite prominent, including:
- Enlargement of forehead and jaw, widening the spaces between teeth and enlarging tongue
- Enlargement of the nose and lips
-
Deepening of the voice in males
- Skin changes, including:
- Increased number of skin tags
- Oily skin and excessive sweating
- Carpal tunnel syndrome, due to increase tissue in the wrists, leading to nerve compression
- Sleep apnea
- Arthritis
- Headache
Serious conditions related to longstanding, untreated acromegaly, include:
- High blood pressure
- Diabetes mellitus (adult-onset or Type 2)
- Heart disease, including heart failure due to heart enlargement
Acromegalic patients are at increased risk of developing other tumors or lesions of the body:
- Thyroid cancer occurs at a higher frequency; speak to your doctor about screening tests.
- Colon polyps; you may need regular colonoscopies to screen for polyps.
If a pituitary growth hormone producing tumor develops in childhood before bone growth is completed, gigantism results. Pituitary giants can grow over seven feet tall.
Acromegaly: Symptoms Related to Large Tumor Size (Macroadenomas)

Macroadenomas that grow upward into the brain cavity can compress the optic chiasm. Vision problems can include:
- A loss of the outer peripheral vision, called a bitemporal hemianopsia
- When severe, a patient can only see what is directly in front of them
- Many patients do not become aware of their visual loss until it is quite severe.
- Other visual problems can include:
- Loss of visual acuity (blurry vision), especially if the macroadenoma grows forward and compresses an optic nerve
- Colors not perceived as bright as usual
Pituitary Failure or Hypopituitarism
- Compression of the normal gland can cause hormone insufficiency, called hypopituitarism. The symptoms depend upon which hormone is involved.
- Reduction of sex hormones, luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
- In men, this can lead to a low testosterone level, causing decreased sexual drive and impotence.
- In some cases, there can be loss of body and facial hair.
- In women, this can lead to infertility.
- In men, this can lead to a low testosterone level, causing decreased sexual drive and impotence.
- Large pituitary tumors can slightly elevate blood prolactin levels. Doctors think this occurs because of compression of the pituitary stalk, the connection between the brain and pituitary gland. It is called the "stalk effect."
- In premenopausal women, this can lead to reduction or loss of menstrual periods and/or breast milk production (galactorrhea).
- Prolactin levels are only slightly elevated, as opposed to prolactinomas in which the prolactin level is usually very high.
More severe hypopituitarism can lead to hypothyroidism or abnormally low cortisol levels, which may be life threatening. Symptoms of severe hypopituitarism include:
- Loss of appetite
- Weight loss or weight gain
- Fatigue
- Decreased energy
- Decreased mental function
- Dizziness
Changes in hormonal function can cause electrolyte imbalance in the blood, typically low sodium levels (hyponatremia). Symptoms could include:
- Fatigue
- Seizures
Acromegaly: Diagnosis
A pituitary adenoma may be suspected based on symptoms, the medical history, and physical findings of acromegaly. Explaining your symptoms is a crucial part of diagnosis, as your doctor uses the information to determine whether a pituitary tumor is secreting an excess of hormones and if there is evidence of pituitary insufficiency. Physicians at the Pituitary Tumor Program at UCLA have vast experience in diagnosing pituitary conditions.
Standard diagnostic tests include:
- Hormone testing
- Imaging scans
Hormone Testing

Doctors will order blood tests, specifically looking for an elevated level of IGF-1. In some rare cases, usually in premenopausal women, the GH levels can be high even though the IGF-1 levels are normal. This is an estrogen-resistant phenomenon.
Normally, the pituitary glands secrete GH in a pulsatile fashion, meaning the level increases and decreases significantly throughout the day. This affects diagnosis in two ways:
- It is difficult to diagnose acromegaly based on a random GH measurement, because a measurement at one time differs drastically from one taken at a different time.
- GH release also falls dramatically after eating a large quantity of sugar, whereas tumor cells do not exhibit this characteristic. This expected drop in hormone production is useful in helping diagnose acromegaly.
IGF-1 is released in a more steady fashion. Its levels do not go up and down quickly, making it a better hormone to measure to screen for acromegaly.
You may be asked to undergo an oral glucose tolerance test (OGTT) to confirm the diagnosis. Drinking 75 grams of a glucose solution should lower the GH level to lower than one nanogram per milliliter. In acromegalics, this suppression does not occur and may in fact increase.
Learn more about hormone testing at the UCLA Pituitary Tumor Program.
Magnetic Resonance Imaging (MRI)
One method we use to detect pituitary tumors is a magnetic resonance imaging (MRI) scan of the pituitary gland. We use a special MRI pituitary protocol to properly visualize the tumor.
Smaller tumors may not be visible using computed tomography (CT) scans.
The vast majority (90%) of GH-secreting tumors are macroadenomas.
Acromegaly: Treatment Options
The optimal treatment of acromegaly depends on multiple factors, including:
- Size and location of the tumor
- Age and medical condition of the patient
Invasive tumors may not be able to be cured surgically.
Typically, more than one specialist is involved in managing pituitary adenomas. At the Pituitary Tumor Program, your medical team includes a special endocrinologist called a neuro-endocrinologist who has specific expertise in the treatment of acromegaly.
Treatment options include:
Acromegaly Treatment: Surgery

Your doctor may recommend surgically removing the tumors as your best chance for a cure. If the tumor invaded beyond the sella (the space where the normal pituitary gland sits), however, there is a lower chance of a surgical cure. In that case, your doctor may recommend other treatment options, such as medication or radiation therapy.
Patients should strongly consider seeking the care of an experienced neurosurgeon, one whom performs a large number of pituitary surgeries each year. Studies have shown:
- The first surgery offers the greatest chance of cure, while the cure rate with a second or third surgery is much lower.
- Newer surgical techniques, such as the expanded, endoscopic endonasal approach allow surgeons to cure pituitary tumors previously thought to be unresectable (unable to be removed surgically).
- Long-term cure of acromegaly after surgery occurs in approximately 80 percent to 85 percent of patients with smaller tumors (microadenomas) and in approximately 50 percent to 60 percent of patients with larger tumors (macroadenomas).
If the pituitary adenomas require surgery, typically the best procedure is through a nasal approach. Our neurosurgeons who specialize in pituitary tumor surgery are experts in the minimally invasive endoscopic endonasal technique. This procedure removes the tumor while minimizing complications, hospital time and discomfort. This advanced technique requires specialized training and equipment.
Very large tumors that extend into the brain cavity may require opening the skull (craniotomy) to access the tumor. Our surgeons are also experts in the minimally invasive "key-hole" craniotomy, utilizing a small incision hidden in the eyebrow.
Acromegaly Treatment: Medication

In recent years, the medical treatment of acromegaly has improved. In some cases, doctors use medication, and not surgery, as the first course of treatment. However, in many cases, patients require both medical and surgical therapies to control acromegaly.
Medications include:
- Somatostatin analog (Octreotide, Lanreotide) injections, typically administered to patients on a monthly basis, suppress growth hormone production in about 70 percent of patients.
- Significant tumor shrinkage occurs in 30 to 50 percent of patients.
- Injections often improve symptoms of soft tissue swelling, headache, joint pains and sleep apnea.
- Patients require lifelong treatment with somatostatin.
- Drugs that block the action of growth hormone on liver cells, such as a daily injection of Pegvisomant. When effective, IGF-1 levels can normalize, but elevated growth hormones remain.
- Drugs that mimic the effect of dopamine, such as cabergoline, are effective in a small number of patients. These medications are the same ones used to treat prolactinomas.
Acromegaly Treatment: Radiation Therapy

For some patients, surgery or medication is not sufficient to control the acromegaly. In these cases, doctors may recommend stereotactic radiosurgery. Stereotactic radiosurgery is a technique in which doctors aim a highly focused dose of radiation to the tumor. It takes an average of 18 months to lower the GH and IGF-1 levels.
The radiation beam is designed to target only the tumor. The surrounding brain structures receive only a fraction of the radiation dose and are typically unharmed, with the exception of the normal pituitary gland.
A consequence of radiation treatment is that it can cause delayed pituitary failure. This typically occurs several years after treatment, and therefore continued long-term follow-up with an endocrinologist is important. Hormone replacement may be required.
Clinical Trials
The UCLA Pituitary Tumor Program has clinical trials testing newer medications for the treatment of acromegaly.
Contact Us
To schedule an appointment with one of our physicians at the Pituitary Tumor Program, please call (310) 825 5111.
You can also email us at [email protected]