Breast MRI Findings: Post-Surgical Findings
by Josh Arnold, MD and Anne Hoyt, MD
Introduction
The detection of breast cancer recurrence following surgery may be challenging from both a clinical and imaging standpoint; breast MRI plays an increasing role in these cases. Most commonly, MRI is performed following breast conservation therapy (BCT). It is important to recognize expected MRI findings following lumpectomy and radiation, as well as suspicious findings which may prompt biopsy.
In some cases, MRI may be performed following mastectomy. Knowledge of the normal post-surgical appearance of mastectomy and various types of reconstruction is key in recognizing recurrent disease.
Imaging Following Breast Conservation Therapy
Post-Surgical Scar
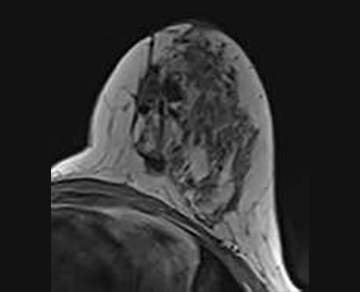
Architectural distortion at the lumpectomy site is an expected finding, and represents a benign (BI-RADS 2) post-surgical scar (Figure 1). Surgical clips will appear as foci of metallic susceptibility artifact.
Seroma
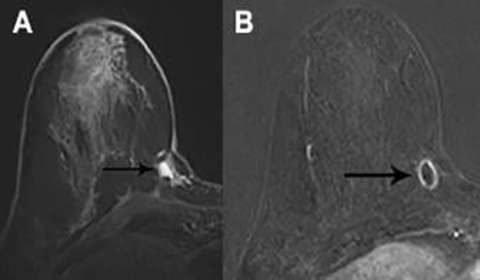
A fluid- or blood-filled cavity following lumpectomy is a normal finding. Seromas are typically T2 hyperintense with smooth, thin rim enhancement (Figure 2a).1 Nodular enhancement greater than 5mm is concerning for residual disease (Figure 2b). A seroma with typical imaging features is a benign finding (BI-RADS 2).
Fat Necrosis
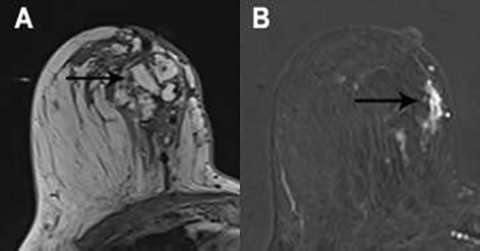
Fat necrosis has a variable imaging appearance, with many cases requiring follow-up imaging (BI-RADS 3) or biopsy (BI-RADS 4).2 Internal fat signal intensity is a classic imaging feature (Figure 3a). Enhancement is variable and may be rim, focal, or diffuse (Figure 3b).3 Calcifications may be seen as signal voids. Correlation with mammography is helpful in identifying central fat density as well as the typical calcifications seen in fat necrosis.
Non-mass Enhancement
Minimal non-mass enhancement (NME) adjacent to the lumpectomy site can be a normal finding up to 18 months following surgery4. A small enhancing focus or minimal linear NME may be appropriate for 6-month imaging follow-up (BI-RADS 3).
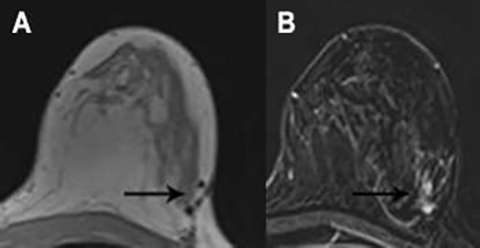
Other than the above, NME within or adjacent to the lumpectomy site is generally suspicious (BI-RADS 4). This includes new or increasing NME, nodular NME measuring greater than 5 mm, mass like enhancement, and NME in suspicious distributions such as segmental, clumped, or regional (Figure 4a and 4b)5. Enhancement kinetics are an important component of the evaluation of NME. Rapid initial enhancement and washout are most concerning for malignancy.
Enhancing Masses
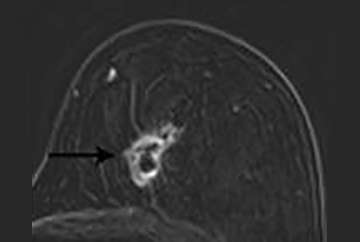
A new enhancing mass (Figure 5), especially those with irregular or spiculated margins, are highly suspicious (BI-RADS 4 or 5).
Imaging Following Mastectomy:
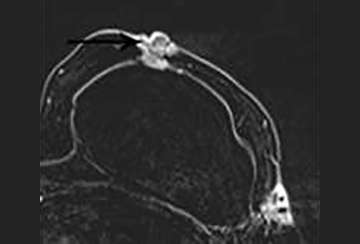
The normal appearance following mastectomy is dependent on the type of reconstruction techniques include autologous tissue flaps and implant reconstruction. Autologous tissue flaps include the transverse abdominis myocutaneous (TRAM) and deep inferior epigastric perforator (DIEP) flaps, although numerous other techniques exist. In general, post-surgical changes such as seromas and fat necrosis will also be encountered following mastectomy as in breast conservation surgery. Recurrences are most common in the anterolateral breast and axilla, where residual breast tissue may remain (Figure 6)6,7.
Conclusion:
Breast MRI may be useful to assess for residual disease or recurrence following breast conservation therapy or in some cases following mastectomy. It is important to recognize benign findings such as a post-surgical scar and seroma. Fat necrosis has a variable imaging appearance and may require imaging follow-up, correlation with mammography, and/or biopsy. Suspicious findings following surgery include new NME, especially in a masslike or ductal pattern, and enhancing masses.
References
- Orel SG, Reynolds C, Schnall MD, Solin LJ, Fraker DL, Sullivan DC. Breast carcinoma: MR imaging before re-excisional biopsy. Radiology 1997;205(2): 429–436. DOI: 10.1148/radiology.205.2.9356624
- Daly CP, Jaeger B, Sill DS. Variable appearances of fat necrosis on breast MRI. AJR Am J Roentgenol 2008;191(5):1374–1380. DOI: 10.2214/AJR.07.4051
- Drukteinis JS, Gombos EC, Raza S, Chikarmane SA, Swami A, Birdwell RL. MR imaging assessment of the breast after breast conservation therapy: distinguishing benign from malignant lesions. Radiographics. 2012 Jan-Feb;32(1):219-34.DOI: 10.1148/rg.321115016
- Li J, Dershaw DD, Lee CH, Joo S, Morris EA. Breast MRI after conservation therapy: usual findings in routine follow-up examinations. AJR Am J Roentgenol 2010;195(3):799–807. DOI: 10.2214/AJR.10.4305
- Schnall MD, Blume J, Bluemke DA, DeAngelis GA, DeBruhl N, Harms S, Heywang-Köbrunner SH, Hylton N, Kuhl CK, Pisano ED, Causer P, Schnitt SJ, Thickman D, Stelling CB, Weatherall PT, Lehman C, Gatsonis CA. Diagnostic architectural and dynamic features at breast MR imaging: multicenter study. Radiology 2006;238(1): 42–53. DOI: 10.1148/radiol.2381042117
- Peng C, Chang CB, Tso HH, Flowers CI, Hylton NM, Joe BN. MRI appearance of tumor recurrence in myocutaneous flap reconstruction after mastectomy. AJR Am J Roentgenol. 2011 Apr;196(4):W471-5. DOI: 10.2214/AJR.10.5279
- Pinel-Giroux FM, El Khoury MM, Trop I, Bernier C, David J, Lalonde L. Breast reconstruction: review of surgical methods and spectrum of imaging findings. Radiographics. 2013 Mar-Apr;33(2):435-53. DOI: 10.1148/rg.332125108