Radiology
Mammography: Calcifications
by Phoebe Ann, MD, Fadi Dahoud, and Anne Hoyt, MD
Introduction
Calcifications occur in the breast in varying morphology and distribution; some indicate benignity while others indicate malignancy. The American College of Radiology Breast Imaging Reporting and Data System (BI-RADS) 5th edition categorizes calcifications into typically benign and suspicious morphology, as described below.
The typically benign calcifications include the following:
- Skin calcifications
- Vascular calcifications
- Coarse or popcorn-like
- Large rod-like
- “Rim” calcifications
- “Round” calcifications, which include the previously described “round” and “punctate” calcifications
- Dystrophic
- Milk of calcium
- Suture
The calcifications with suspicious morphology include the following:
- Amorphous
- Coarse heterogeneous
- Fine pleomorphic
- Fine linear or fine linear branching
Distribution of calcifications include the following:
- Diffuse
- Segmental
- Regional
- Grouped
- Linear
Typically Benign Calcifications
Skin calcifications: often polygonal calcifications with radiolucent center
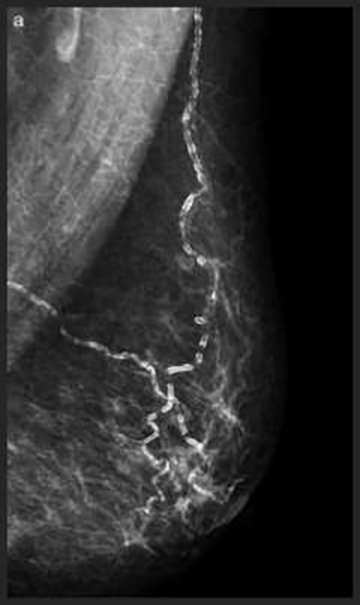
Vascular calcifications: parallel calcifications outlining the vessel wall
|
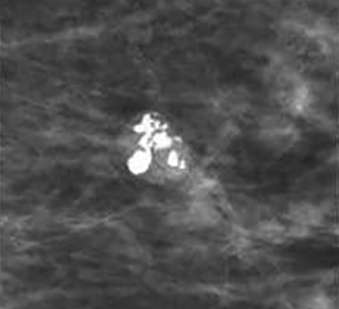
Coarse or popcorn-like calcifications: dense calcifications larger than 2-3 mm, often coalescing over time and indicative of hyalinizing fibroadenoma

Large Rod-like Calcifications: thick calcifications which follow the ducts, toward the nipple, secondary to secretory disease
|
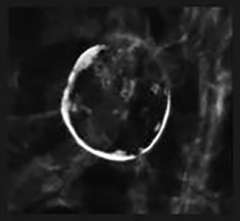
Rim Calcifications: Include the previously described “eggshell” and “radiolucent centered” calcifications. These correspond to calcifications along round lesions such as oil cysts or simple cysts. These are usually associated with history of trauma or surgery.

Round Calcifications: Include the previously described “round” and “punctate” calcifications. As the name implies these are round in morphology.
|
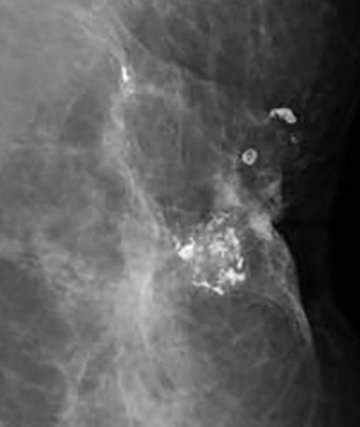
Dystrophic Calcifications: thick, usually greater than 1 mm, rough and irregular calcifications which tend to coalesce. They are a manifestation of fat necrosis in response to trauma or surgery and are often located along surgical scar tissue as seen below.
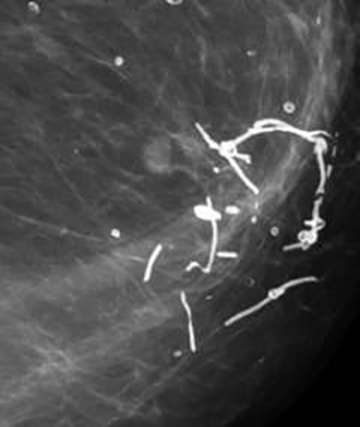
Suture Calcifications: These represent calcium deposited within suture material, and appear linear or tubular and may outline surgical knots.
|
Milk of Calcium Calcifications: Craniocaudal View
Milk of Calcium Calcifications: True Lateral Views
|
Calcifications with Suspicious Morphology
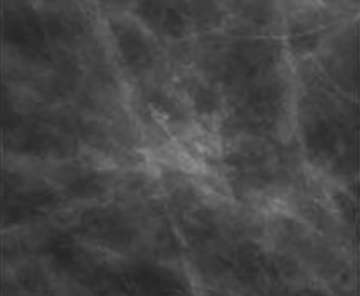
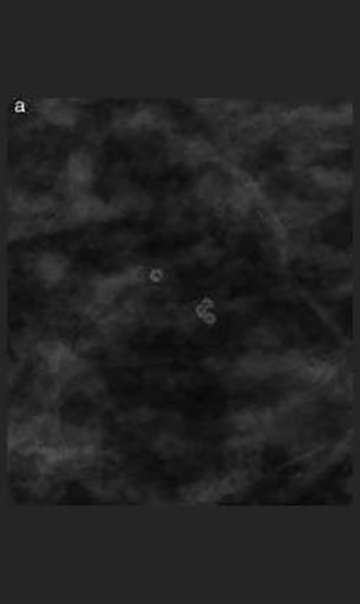
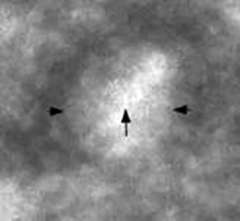
Amorphous calcifications: calcifications that are so small and faint that their shapes are not appreciable, amorphous calcifications are considered a 4B category finding.

Coarse heterogeneous calcifications: irregular and defined calcifications which often coalesce, coarse heterogeneous calcifications usually measure more than 0.5 mm but less than the dystrophic calcifications. One lone group of coarse heterogeneous calcifications is considered a 4B category finding.
|

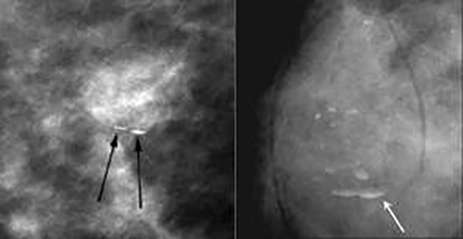
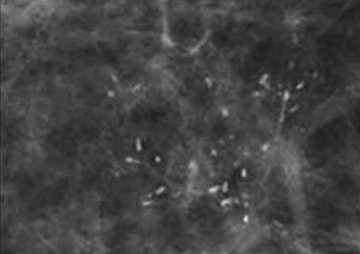
Fine pleomorphic calcifications: calcifications of different shapes and sizes, with a size between 0.5 and 1.0 mm, smaller than coarse heterogeneous calcifications. These are considered a 4B category finding.
Fine linear or fine linear branching: thin, linear and usually discontinuous calcifications which represent calcified necrotic debris within a duct compromised by carcinoma. When these calcifications are new and present in a segmental distribution, they are considered a BIRADS 5 category finding.
|
Distribution
- Distribution of calcifications include the following:
- Diffuse: random distribution throughout the breast, considered benign
- Regional: calcifications cover an extensive area, more than one quadrant
- Grouped/clustered: at least 5 calcifications within 1 cm, often requiring further evaluation.
- Linear: calcifications arranged in a linear path that can branch, suggesting calcified debris within a duct. These require further evaluation.
- Segmental: calcifications follow the anatomic triangular shape of a breast lobe with tip towards the nipple. These require further evaluation.
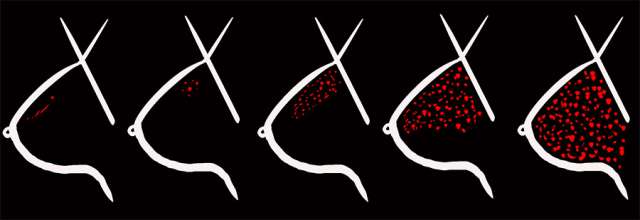
From left to right: linear, grouped, segmental, regional, and diffuse.
References
- Nalawade YV. Evaluation of breast calcifications. Indian J Radiol Imaging. 2009 Oct-Dec;19(4):282-6. DOI: 10.4103/0971-3026.57208.
- Rao AA, Feneis J, Lalonde C, Ojeda-Fournier H. A Pictorial Review of Changes in the BI-RADS Fifth Edition. Radiographics. 2016 May-Jun;36(3):623-39. DOI: 10.1148/rg.2016150178.
- Hernandez PLA, Estrada TT, Pizarro AL, Cisternas MLD, Tapia CS. Breast calcifications: description and classification according to BI-RADS 5th Edition. Revista Chilena de Radiologia 2016; 22(2): 80-91.
- Muttarak M, Kongmebhol P, Sukhamwang N. Breast calcifications: which are malignant? Singapore Med J. 2009 Sep;50(9):907-13; quiz 914. PMID: 19787181