Aneurysm
Find your care
Our expert team is skilled at treating complex cerebrovascular conditions and providing the finest and most comprehensive patient care. For help finding a neurosurgeon, call 310-825-5111.
Overview
What is a brain aneurysm?
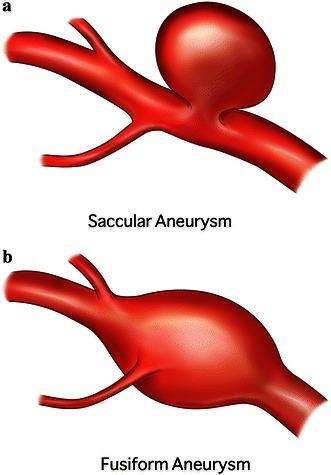
An aneurysm, also called a cerebral aneurysm or intracranial aneurysm, is an area of weakness in the wall of a brain artery. Over time, the weak spot can grow and begin to balloon out from the artery. This bulge is called an aneurysm (Figure 1).
Signs and Symptoms
What are the symptoms of an aneurysm?
People with unruptured aneurysms often have no symptoms, especially if the aneurysm is still small. If an aneurysm grows large enough to impact the brain or press on a nearby nerve, symptoms may develop such as:
- Headache
- Pain above or behind the eye
- Blurred vision or double vision
- Dilated eye pupil
- Numbness or weakness of the face, arm, or leg
Like a balloon, an aneurysm can rupture, leading to bleeding around the brain – a condition called a subarachnoid hemorrhage (SAH). SAH is a type of stroke, and it is classified as a hemorrhagic (bleeding) stroke. This is a very serious condition that must be treated immediately. Symptoms of a ruptured aneurysm come on suddenly, and can include any of the above symptoms, but more frequently involves the following:
- Sudden, severe headache often described as the “worst headache of my life”
- Nausea or vomiting (after the rapid, severe headache)
- Seizure
- Loss of balance
- Difficulty speaking
- Loss of consciousness
If you or someone you are with experience any of these symptoms, Call 911 or your local emergency number immediately. Don't wait to see if symptoms go away. The longer the time before stroke treatment, the greater the chance of brain damage and disability.
Diagnosis
How are brain aneurysms diagnosed?
At UCLA, we use the most advanced imaging technologies to diagnose brain aneurysms quickly and accurately. In some cases, an aneurysm is only discovered once it has ruptured, but we do everything possible to diagnose and manage them before they rupture. During your examination, your expert team may use any of the following imaging techniques to locate and assess your aneurysm:
- Magnetic resonance angiography (MRA)is a non-invasive test that uses magnetic resonance (MR) technology to create images of blood vessels in the brain. This study can be done with or without contrast dye, depending on type of images sought.
- Computed tomography angiography (CTA)is a non-invasive test that uses injected contrast dye and CT scanning to identify abnormalities of the brain blood vessels.
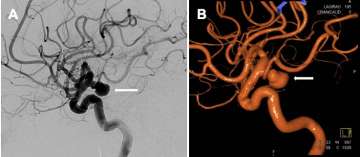
- Cerebral digital subtraction angiography (catheter angiography)is a procedure in which physicians advance small tubes inside the blood vessels and inject contrast dye through these tubes to provide very detailed images of the blood vessels of the brain. This allows them to precisely identify the location, size, and shape of the aneurysm, as well as to assess many other important features of the anatomy and blood flow to the brain. Cerebral angiography is the highest quality test to analyze the blood vessels of the brain, spine and neck. It is considered the “gold standard” for imaging of brain aneurysms, and gives the best images of any imaging modality. Figure 2 demonstrates examples of images from a cerebral angiogram.

Treatment
How are brain aneurysms treated?

Following your diagnosis, you and your team of cerebrovascular specialists will discuss the options for treatment and management of your aneurysm. We will fully customize a treatment plan based on your age, overall health, size, location and shape of the aneurysm. Often, there is more than one way to treat a brain aneurysm. These options will be discussed with you in detail so that you understand all the relevant options and so that we can determine the best option specifically for you.
Treatment options for aneurysms are numerous and are constantly being improved. The UCLA cerebrovascular team has a long history of technological development and testing innovative devices in clinical trials. Patients will be evaluated for newer treatments and clinical trials as appropriate. An overview of common treatment options include, but are not limited to:
- Non-surgical monitoring: Some aneurysms are considered low risk of rupture or other problems. If your aneurysm does not require immediate treatment, we will create a customized monitoring plan, watching it closely and regularly while managing any specific risk factors that you might have.
-
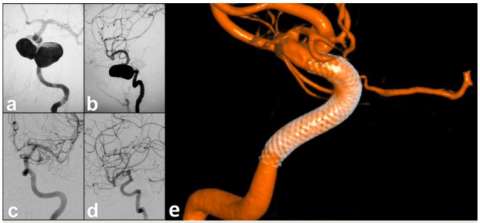 Figure 5. Flow Diversion Treatment of a giant left internal carotid artery cavernous segment aneurysm - pre-treatment (a) AP and (b) lateral angiographic views demonstrating the giant aneurysm before treatment. Six months post-treatment
Figure 5. Flow Diversion Treatment of a giant left internal carotid artery cavernous segment aneurysm - pre-treatment (a) AP and (b) lateral angiographic views demonstrating the giant aneurysm before treatment. Six months post-treatmentEndovascular surgery: Endovascular surgery techniques are performed using a catheter(s) inserted through an artery in the groin or the wrist/arm. The catheters are navigated to the blood vessels of the brain, where the aneurysm is then treated through these catheters. This avoids open surgery on the brain, and speeds recovery. Endovascular techniques used to treat aneurysms are numerous and include:
- Coiling: Using techniques developed at UCLA, small platinum wires called coils are placed into the aneurysm to seal it off and prevent blood flow into it. Coiling is sometimes performed with balloons or stents designed to hold coils in place. The Guglielmi detachable coils (GDCs) that are now standard for treating complex aneurysms were invented at UCLA (Figures 3, 4A, and 4B).
- Flow diversion: In this technique, a stent(s) is inserted into the artery that the aneurysm arises from to divert blood flow away from the aneurysm so that the blood vessel wall may heal. The inner lining of the blood vessel (the endothelium) grows onto the stent to seal off the opening of the aneurysm and prevent flow into the aneurysm. This technique was originally developed for treatment of large and giant aneurysms, but it has since been adapted for aneurysms of various shapes, sizes, and locations (Figure 5).
-
 Figure 6. Intrasaccular flow disruption of an ICA terminus aneurysm using the WEB device. Top panel demonstrates sequential images from left to right showing deployment and finally detachment of the WEB device
Figure 6. Intrasaccular flow disruption of an ICA terminus aneurysm using the WEB device. Top panel demonstrates sequential images from left to right showing deployment and finally detachment of the WEB deviceIntrasaccular flow disruption: This technique involves placement of a special braided mesh device (for example, the WEB device) inside the aneurysm in order to block blood flow into the aneurysm. This technique is especially good for aneurysms located at branch points in the vessel, so called bifurcation aneurysms (Figure 6).
- Parent vessel occlusion: This technique, in which surgeons block the vessel feeding blood to the aneurysm, is more rarely used as a method for stopping blood flow into the aneurysm.
- Microsurgery: At UCLA, we frequently employ minimally-invasive “keyhole” access techniques to surgically treat brain aneurysms. There are then several open microsurgical techniques that may be used to treat aneurysms, including but not limited to:
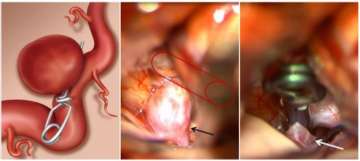
- Microsurgical clipping: In this technique, the neurosurgeon places a titanium clip across the neck/base of the aneurysm to cut off blood flow into the aneurysm, eliminate pressure on the aneurysm, and to prevent rupture. This is technique with excellent long-term outcomes, and it has been continuously refined over the years since its first use in the 1930s (Figure 7).
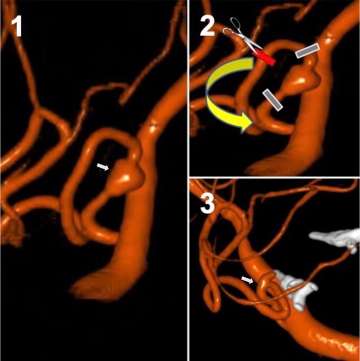
- Aneurysm trapping and bypass: Open surgery is used to trap (block/exclude) the weak area of the vessel containing the aneurysm. A bypass is then performed to redirect blood flow around the trapped aneurysm, thereby keeping the vessel beyond the occlusion flowing, and preventing brain damage. This technique has many nuances to it and is customized based on patient-specific anatomy and blood flow needs (Figure 8).
- Wrapping: This technique involves wrapping the aneurysm in fabric to support it and help prevent rupture. Wrapping is typically used in combination with microsurgical clipping, but it can be used as a treatment if other options are not suitable.
Postoperative care and recovery
Brain aneurysm diagnosis and treatment procedures are performed at Ronald Reagan UCLA Medical Center. The postoperative care and recovery will depend on the type of treatment performed. Since the procedures are performed using cutting edge technologies and often use minimally invasive technique, there is commonly reduced discomfort and a shortened hospital stay compared to traditional treatments. After treatment, patients are commonly monitored overnight in the hospital and may be discharged as early as the following day.
At UCLA Health neurosciences, we employ highly specialized multidisciplinary health care teams, and in addition to innovative cutting-edge care, we provide support services for patients and their families to help navigate their time in our clinics and hospitals.
Contact us
To schedule an appointment at the UCLA Cerebrovascular Program, please call 310-825-5111 or request a call back for an appointment.

Geoffrey Colby, MD, PhD

Jeremiah Johnson, MD
