Middle Meningeal Artery Embolization for Chronic Subdural Hematoma
Find your care
Our expert team is skilled at treating complex cerebrovascular conditions and providing the finest and most comprehensive patient care. For help finding a neurosurgeon, call 310-825-5111.
Overview
What is a chronic subdural hematoma (cSDH)?
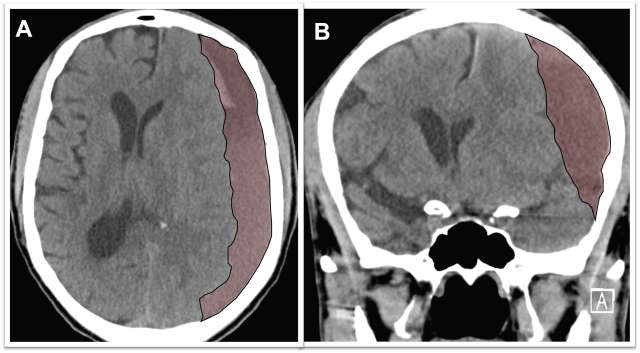
Chronic subdural hematoma (cSDH) is a collection of degrading blood products in the space between the surface of the brain and the inner lining of the skull, called the “dura mater.” These types of collections occur more frequently in older age groups due to the increased space between the brain surface and the dura mater as we age. Chronic subdural hematoma collections are thought to begin as relatively small bleeds after a minor event such as bumping of the head, but over time, the collections can grow, particularly in patients who have other reasons to bleed such as use of blood thinners or other medical reasons. If they become large enough, they create pressure on the brain and result in symptoms (Figure 1).
Symptoms
What are the symptoms of chronic subdural hematoma?
Symptoms from chronic subdural hematomas are often mild such as headaches but over time may slowly increase to include behavioral changes such as confusion or atypical behavior. As time passes, these lesions can cause further pressure on the brain leading to weakness on one side of the body, inability to walk, seizures and even coma.
- Headache
- Confusion
- Seizures
- Weakness on one side of the body
- Imbalance
Why do chronic subdural hematomas grow?
After a bleed in the subdural space, the body attempts to remove the blood collection by forming a thin layer around it called subdural membranes. The membranes contain tiny vascular channels which allow the body’s immune system to break down and remove the blood that has leaked into the subdural space. However, these small vessels in the membrane are also famously leaky, and in some patients, the membranes bleed little by little into the subdural space faster than the membranes can absorb the initial blood clot. The net effect of this process is growth of hematoma over weeks to months until it becomes large enough to cause symptoms.
Risk Factors
What are the risk factors for developing a chronic subdural hematoma?
Though the causes of chronic subdural hematoma are not always clear, certain factors may increase your risk of having the condition, including:
- Mild Head Injury. Chronic subdural hematomas commonly develop in the setting of a recent fall or minor head injury in an older patient or at-risk patient. The head jarring is believed to initiate a subdural hemorrhage that can grow with time.
- Advanced Age. The older age groups are more at risk of developing chronic subdural hematoma due to brain volume reduction that is natural with ageing but allows more space between the brain surface and skull for chronic subdural hematomas to accumulate.
- Blood Thinner (anticoagulant and antiplatelet) Medications. Blood thinner medications increase the risk of bleeding in the space above the brain and below the dura (subdural space). Once a chronic subdural hematoma is detected, blood thinners are typically stopped to reduce the risk of hematoma expansion.
- Medical conditions. Certain medical conditions such as liver failure or renal failure can lead to poor blood clotting and increase the risk of bleeding.
- Dementia. Patients with dementia often have significantly reduced brain volume (brain atrophy) and are at risk of falls. This makes them higher risk for developing chronic subdural hematomas.
Consultation at UCLA
UCLA neurosurgeons utilize the latest tools and techniques to diagnose and treat chronic subdural hematomas.
Tests to diagnose chronic subdural hematomas may include:
- CT Scan Brain – the most commonly and most useful diagnostic test for chronic subdural hematoma. New bleeding events are quickly and reliably identified by CT imaging.
- MRI Brain – can see brain structures in more detail. Helpful for identifying bridges in the membranes called septations. The presence of many septations may influence the treatment options and recommendations.
Treatment
How are chronic subdural hematomas treated?
Classically, treatment of chronic subdural hematomas was either with observation or surgical drainage of the blood products. These are the best management option for many patients. However, there is an alternative chronic subdural hematoma treatment option called Middle Meningeal Artery (MMA) Embolization which has demonstrated good results resolving chronic subdural hematomas without open surgery in select patients.
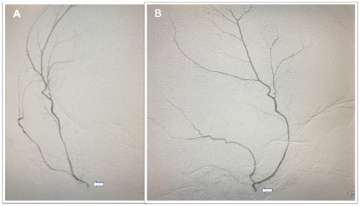
Middle Meningeal Artery Embolization – This procedure is performed in an endovascular suite with the patient asleep under general anesthesia. The endovascular surgeon uses minimally invasive technique to enter the blood vessels in the arm or leg and then advances small tubes called catheters through the arteries under x-ray guidance to the middle meningeal artery on the side of the subdural hematoma. The middle meningeal artery is located on the underside of the skull (outside of the brain) but also provides blood supply to the abnormal membranes that surround the hematoma and contribute to hematoma growth (Figure 2). Under fluoroscopic guidance, the surgeon delivers a specially made liquid glue material (called nBCA or Onyx) or small particles through the small tube and permanently blocks the middle meningeal artery. Platinum micro-coils can be used as well. After the procedure, the tubes are removed and the small puncture site in the arm or leg artery is closed. In the weeks following the procedure, there is reduced bleeding from the subdural hematoma membranes and the hematoma collection slowly shrinks in size and often goes away completely over the course of several months (Figure 3).
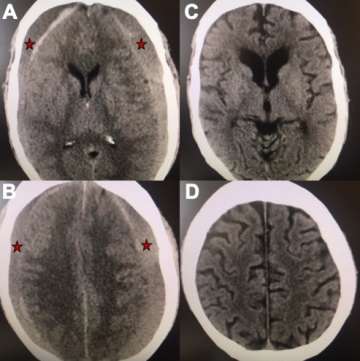 Figure 3. A, B) Axial views of a brain CT scan demonstrating chronic subdural hematomas on both sides of the brain compressing it inwards (red stars mark the hematoma). C, D) Axial views of a CT brain of the same chronic subdural hematoma 3 months after Middle Meningeal Artery Embolization demonstrating resolution of the chronic subdural collection on both sides.
Figure 3. A, B) Axial views of a brain CT scan demonstrating chronic subdural hematomas on both sides of the brain compressing it inwards (red stars mark the hematoma). C, D) Axial views of a CT brain of the same chronic subdural hematoma 3 months after Middle Meningeal Artery Embolization demonstrating resolution of the chronic subdural collection on both sides.- Burr hole Drainage – This is the most common surgical procedure for treatment of chronic subdural hematomas and is performed in the operating room with the patient under general anesthesia. The procedure involves opening two holes, each about the size of a quarter, in the skull to evacuate (drain) the hematoma. A drain is often left in the hematoma space for several days after surgery to maximize the drainage.
- Craniotomy – This procedure is performed in the operating room by opening a larger area of the skull and directly removing the chronic subdural hematoma with surgical instruments and drainage. The procedure is best for surgical removing some of the subdural membranes. A drain is often left in the hematoma space for several days after surgery to maximize the drainage.
Post-operative care and recovery
Middle meningeal embolization procedures for chronic subdural hematoma treatment are performed at Ronald Reagan UCLA Medical Center. Since the procedures are performed using minimally invasive technique, patients experience reduced discomfort and a shortened hospital stay compared to traditional surgery. After treatment, patients are monitored overnight in the hospital and may be discharged as early as the following day. At UCLA Health neurosciences, we employ highly specialized multidisciplinary health care teams, and in addition to innovative cutting-edge care, we provide support services for patients and their families to help navigate their time in our clinics and hospitals.
Contact us
To schedule an appointment at the UCLA Cerebrovascular Program, please call 310-825-5111 or request a call back for an appointment.

Geoffrey Colby, MD, PhD

Jeremiah Johnson, MD
