Architectural Distortion
by Ashley Yeager, MD, Lucy Chow, MD, and Bo Li, MD
Definitions
Architectural distortion is a descriptive term used by radiologists to describe a particular mammogram finding related to the appearance of the breast tissue. The Breast Imaging Reporting and Data System (BI-RADS) is a tool which sets guidelines for radiologists to assess the risk of various breast findings. This system defines architectural distortion as breast parenchyma that is “distorted with no definite mass visible. This includes spiculations radiating from a point and focal retraction or distortion at the edge of the parenchyma.”1
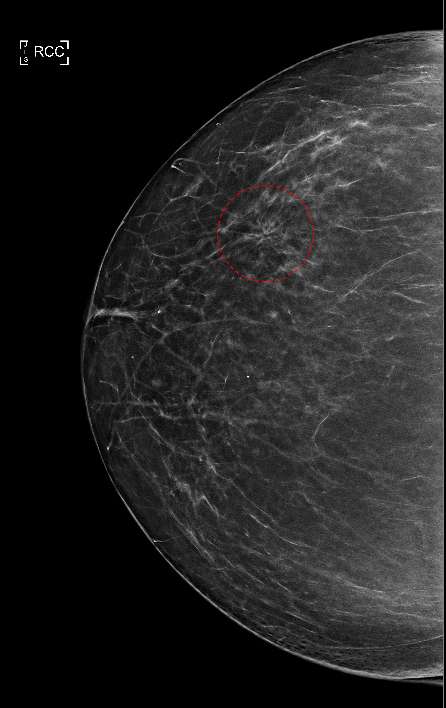
Figure 1 shows a classic mammogram appearance of architectural distortion. As denoted by the red circle, abnormal, fine tissue lines can be seen emanating in a radial pattern and appear to originate from a central focal region. This is in contrast to the surrounding normal parenchymal breast tissue which does not follow this irregular radial pattern. Architectural distortions may be present with no additional mammogram findings (as seen in Figure 1) or in association with other findings such as calcifications or dense masses.
When initially found on 2D digital screening mammogram, additional mammographic imaging with tomosynthesis including with spot-compression is warranted. Several studies have shown that detection of architectural distortion improves with tomosynthesis2,3 by allowing visualization of the breast in thin, sequential sections. Visualizing a lesion of interest as multiple sequential planes can help the radiologist rule out the possibility that the lesion merely represents superimposition of overlapping normal breast tissue which occurs commonly when a 3-dimensional tissue is represented as a 2-dimensional image.2
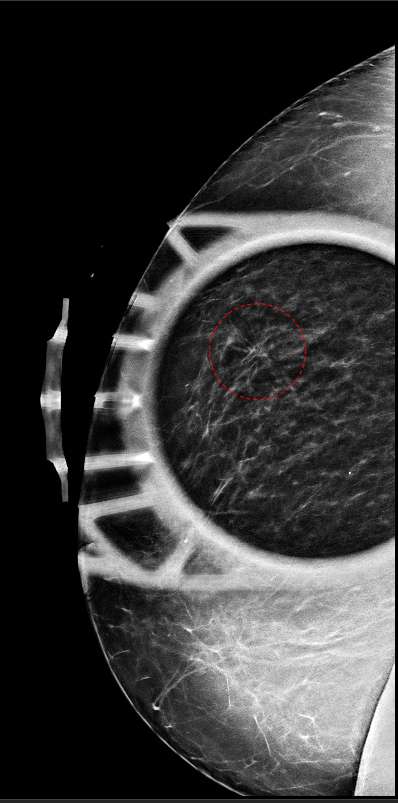
Figure 2 shows spot compression tomosynthesis of the architectural distortion shown in Figure 1. Note how the region of architectural distortion does not appear to “smooth out”, but rather retains a fairly stable appearance compared to Figure 1.
Architectural distortion often represents a diagnostic challenge as it can be a subtle finding and has been reported as the most commonly missed abnormality on traditional 2D digital screening mammograms.4 The advent of 3D tomosynthesis has improved the detection of architectural distortion compared to traditional 2D mammographic views,5 however, this increased detection rate has also translated to an increased false positive rate and a reported positive predictive value for malignancy of just over 50%.5
Causes
Architectural distortion can be caused by both benign and malignant entities. Shaheen et al. recently classified architectural distortions based on their causality and categorized these into groups termed “Apparent,” “Primary” or “Secondary”. Apparent architectural distortions are those distortions that do not persist with additional mammogram views and represent the overlap of normal breast tissue.6
Primary architectural distortions include lesions that arise within the breast de novo without an identifiable cause. These lesions include: both malignant and benign primary breast cancers, fibrosis and radial sclerosing lesions, sclerosing adenosis, and mesenchymal neoplasms arising from mammary stroma tissues.6
Secondary architectural distortions are lesions which arise due to causes that are known to distort breast tissues. The most common entities include those tissue changes which occur following breast surgeries such as lumpectomy/excision or cosmetic surgeries such as reduction mammoplasty, as well as known traumatic injuries to the breast and changes associated with some breast infections.6
Architectural distortions often do not have a sonographic correlate. However, recent advances in sonography have allowed some researchers to correlate some malignancy-associated architectural distortions with key sonographic findings. Takei et al. recently reported ultrasound findings correlating with architectural distortions. Findings included retraction of surrounding breast tissue adjacent a malignancy, the actual malignancy itself, tumor spreading into the Cooper ligaments of the breast, and fibrosis caused by contraction of breast tissue following chemotherapy.7
Management
The malignancy risk associated with architectural distortion varies widely within the literature and researchers have reported positive predictive values ranging from 10%8 to over 50%5 when found by digital breast tomosynthesis. Architectural distortion is considered a high risk entity and has been reported to represent the third most common finding of non-palpable breast cancers.9
Architectural distortions associated with other findings, such as a distinct mass-like lesion or calcifications, are typically considered higher risk regardless of whether the additional finding was seen by ultrasound or mammography. Several researchers have reported a nearly 3-fold malignancy risk for architectural distortions that have an associated sonographic finding compared to those without a sonographic correlate.10,11 These are commonly referred for biopsy via stereotactic-guided mammogram or ultrasound with pathological outcomes dictating surgical management.
Architectural distortions with no sonographic correlate or additional mammogram findings can be challenging. Architectural distortion without an associated mass finding is seen more commonly in association with a malignant cause compared to a benign cause.12 Given the relatively high association of architectural distortion with malignant causes, many radiologists will recommend a biopsy and possibly additional surgical management even for those lesions which return as benign entities. This can lead to increased patient morbidity from unnecessary surgical interventions.
Several studies have explored the use of breast MRI to manage architectural distortions when no other associated mammogram or ultrasound findings can be seen. Amitai et al. recently showed that in cases with no sonographic or associated mammogram findings, the negative predictive value for breast MRI reached nearly 100% and authors argued that special cases of architectural distortion with a negative breast MRI could be followed by imaging alone without the need for surgical intervention.13
References
- D’Orsi, C., Sickles, E., Mendelson, E. & Morris, E. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System. (Reston, VA, American College of Radiology, 2013). https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Bi-Rads
- Partyka, L., Lourenco, A. P. & Mainiero, M. B. “Detection of Mammographically Occult Architectural Distortion on Digital Breast Tomosynthesis Screening: Initial Clinical Experience.” Am. J. Roentgenol. 203, 216–222 (2014). DOI: 10.2214/AJR.13.11047
- Yang, T.-L., Liang, H.-L., Chou, C.-P., Huang, J.-S. & Pan, H.-B. “The adjunctive digital breast tomosynthesis in diagnosis of breast cancer.” BioMed Res. Int. 2013, 597253 (2013). DOI: 10.1155/2013/597253
- Burrell, H. C. et al. “Screening interval breast cancers: mammographic features and prognosis factors.” Radiology 199, 811–817 (1996). DOI: 10.1148/radiology.199.3.8638010
- Bahl, M., Lamb, L. R. & Lehman, C. D. “Pathologic Outcomes of Architectural Distortion on Digital 2D Versus Tomosynthesis Mammography.” AJR Am. J. Roentgenol. 209, 1162–1167 (2017). DOI: 10.2214/AJR.17.17979
- Shaheen, R., Schimmelpenninck, C. A., Stoddart, L., Raymond, H. & Slanetz, P. J. “Spectrum of diseases presenting as architectural distortion on mammography: multimodality radiologic imaging with pathologic correlation.” Semin. Ultrasound. CT MR 32, 351–362 (2011). DOI: 10.1053/j.sult.2011.03.008
- Takei, J. et al. “Clinical implications of architectural distortion visualized by breast ultrasonography.” Breast Cancer Tokyo Jpn. 16, 132–135 (2009). DOI: 10.1007/s12282-008-0085-5
- Alshafeiy, T. I. et al. “Outcome of Architectural Distortion Detected Only at Breast Tomosynthesis versus 2D Mammography.” Radiology 288, 38–46 (2018). DOI: 10.1148/radiol.2018171159
- Gaur, S., Dialani, V., Slanetz, P. J. & Eisenberg, R. L. “Architectural distortion of the breast.” AJR Am. J. Roentgenol. 201, W662-670 (2013). DOI: 10.2214/AJR.12.10153
- Bahl, M., Baker, J. A., Kinsey, E. N. & Ghate, S. V. “Architectural Distortion on Mammography: Correlation With Pathologic Outcomes and Predictors of Malignancy.” AJR Am. J. Roentgenol. 205, 1339–1345 (2015). DOI: 10.2214/AJR.15.14628
- Dou, E., Ksepka, M., Dodelzon, K., Shingala, P. Y. & Katzen, J. T. “Assessing the Positive Predictive Value of Architectural Distortion Detected with Digital Breast Tomosynthesis in BI-RADS 4 Cases.” J. Breast Imaging 2, 552–560 (2020). DOI: 10.1093/jbi/wbaa078
- Park, J. W., Ko, K. H., Kim, E.-K., Kuzmiak, C. M. & Jung, H. K. “Non-mass breast lesions on ultrasound: final outcomes and predictors of malignancy.” Acta Radiol. Stockh. Swed. 1987 58, 1054–1060 (2017). DOI: 10.1177/0284185116683574
- Amitai, Y. et al. “Can breast MRI accurately exclude malignancy in mammographic architectural distortion?” Eur. Radiol. 30, 2751–2760 (2020). DOI: 10.1007/s00330-019-06586-x