Case: Architectural Distortion
by Jason Yoon, MD and Anne Hoyt, MD
A 42 year-old patient with history of chronic anemia presented to a primary care physician to establish care since moving to California. The patient had no complaints. The patient denied any breast abnormalities, including palpable masses, skin changes, or nipple discharge. Review-of-systems was negative besides intermittent dizziness. There was no family history of breast or gynecologic cancers. The patient was married with 2 children, with previous history of Cesarean section. The patient reported having an intrauterine device in place. A physical exam was negative, however a clinical breast examination was deferred. A screening bilateral mammogram was ordered as part of general health maintenance.
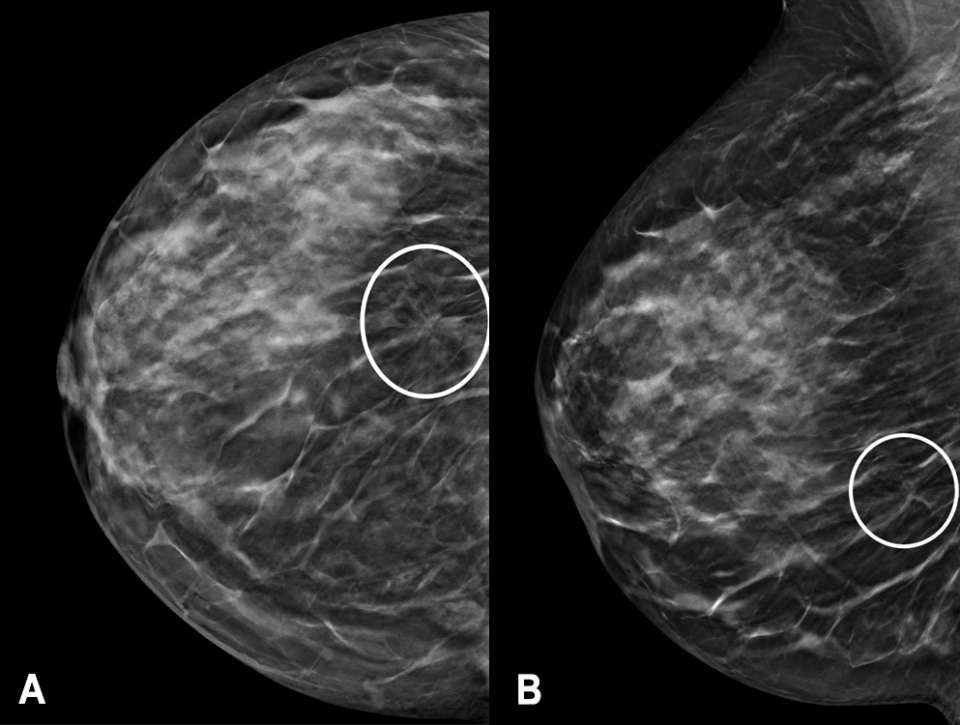
The screening mammogram demonstrated an area of architectural distortion in the lower outer quadrant of the right breast (Figure 1). By the Tyrer-Cuzick version 8 risk calculator, the patient was high-risk, with an approximate 20.3% lifetime risk of developing breast cancer. The mammographic findings were categorized as a BI-RADS 0, and the patient was called back for a diagnostic mammogram with possible diagnostic breast ultrasound.
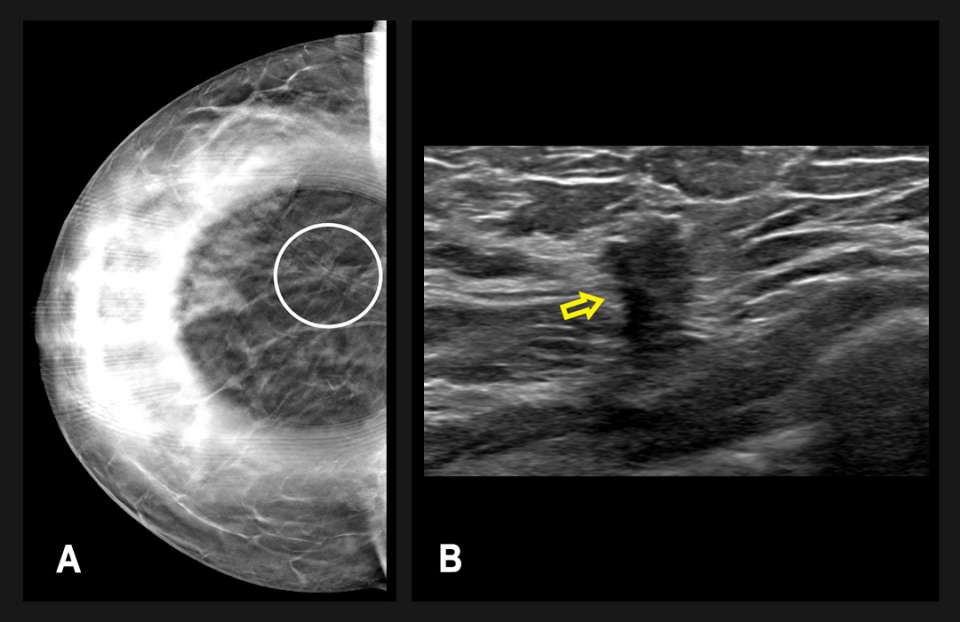
Diagnostic mammography followed one month thereafter and included spot compression views of the area of architectural distortion in the right breast (Figure 2A). Targeted breast ultrasonography showed a vague hypoechoic area measuring up to 11 mm, which correlated with the mammographic findings (Figure 2B). The finding was categorized as BI-RADS 4B, and an ultrasound-guided biopsy was recommended.
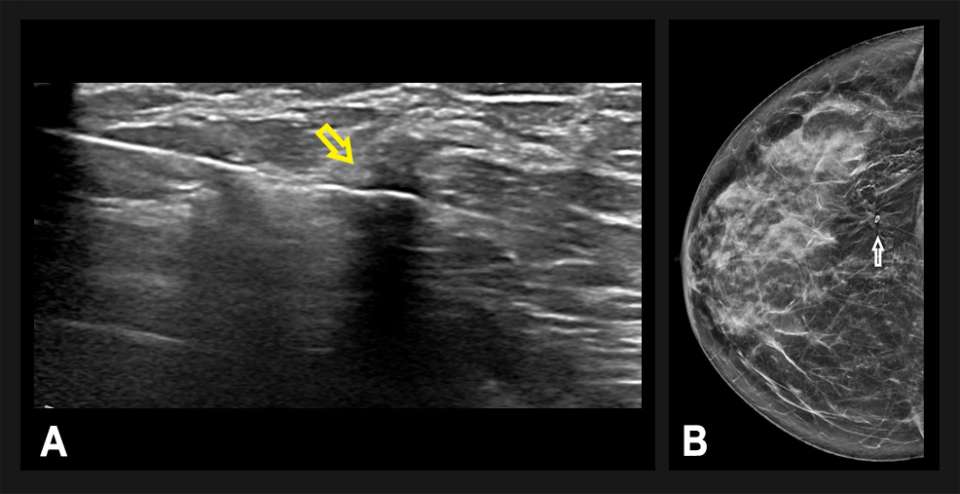
A technically-successful ultrasound-guided biopsy was performed, with 6 core samples obtained (Figure 3). A post-biopsy mammogram confirmed accurate positioning of the biopsy microclip at the site of architectural distortion. Pathology revealed invasive ductal carcinoma, grade 1 estrogen receptor negative, progesterone receptor negative, and HER2 positive. The patient underwent a right breast lumpectomy and sentinel lymph node biopsy, followed by adjuvant radiation.
Discussion
Architectural distortion is described as distorted appearance of the breast parenchymal tissue without an associated mass, often with the appearance of linear densities or spiculations radiating from a central focus.1,2 Additional descriptors included in BI-RADS include focal retraction, straightening, and/or distortion at the edges of the parenchyma.1 Architectural distortion is the third most common mammographic finding of non-palpable breast cancer, reported in up to 4% of screen-detected cancers.3,4 Architectural distortion may also be a secondary finding, associated with masses or calcifications.
Both 2D mammography and digital breast tomosynthesis can reveal architectural distortion, although tomosynthesis is more sensitive.5 With 2D mammography, the positive predictive value for architectural distortion varies from 10-67% for screening and 60-83% for diagnostic examinations.4,5,6 When an architectural distortion is associated with a positive ultrasound finding, such as our case, the likelihood for malignancy is higher.5,6 Invasive ductal carcinoma and invasive lobular carcinoma are the two most common breast cancers associated with architectural distortion, with one retrospective study on pure invasive lobular carcinoma reporting architectural distortion as the most common mammographic finding.3
In addition to malignant etiologies, there are several benign conditions that can result in architectural distortions. Post-surgical (i.e. breast reduction surgery, lumpectomy) and post-biopsy changes are the most common. Other differential considerations include idiopathic proliferative processes such as radial scars or complex sclerosing lesions, fibrotic fat necrosis, or the rare spiculated lesions such as fibromatosis (extra-abdominal desmoid tumor) or granular cell tumor.3 Nevertheless, in the absence of a definitive surgical scar, architectural distortion should undergo biopsy, with stereotactic or tomosynthesis-guided biopsy a viable option when there is no ultrasound correlate.
References
- D’Orsi, Carl, L. Bassett, and S. Feig. "Breast Imaging Reporting and Data System (BI-RADS)." Breast imaging atlas, 4th edn. American College of Radiology, Reston (2018).
- Ikeda, Debra, and Kanae Kawai Miyake. Breast imaging: the requisites. Elsevier Health Sciences, 2016.
- Gaur S, Dialani V, Slanetz PJ, Eisenberg RL. "Architectural Distortion of the Breast." AJR Am J Roentgenol. 2013 Nov;201(5):W662-70. DOI: 10.2214/AJR.12.10153.
- Venkatesan A, Chu P, Kerlikowske K, Sickles EA, Smith-Bindman R. "Positive Predictive Value of Specific Mammographic Findings According to Reader and Patient Variables." Radiology. 2009 Mar;250(3):648-57. DOI: 10.1148/radiol.2503080541.
- Alshafeiy TI, Nguyen JV, Rochman CM, Nicholson BT, Patrie JT, Harvey JA. "Outcome of Architectural Distortion Detected Only at Breast Tomosynthesis Versus 2D Mammography." Radiology. 2018 Jul;288(1):38-46. DOI: 10.1148/radiol.2018171159.
- Bahl M, Baker JA, Kinsey EN, Ghate SV. "Architectural Distortion on Mammography: Correlation with Pathologic Outcomes and Predictors of Malignancy." AJR Am J Roentgenol. 2015 Dec;205(6):1339-45 DOI: 10.2214/AJR.15.14628.