Case: Sternalis Muscle
By: Dan Li, M.D. and Melissa Joines, M.D.
Introduction
The sternalis muscle is an anomalous muscle of the anterior chest wall. It lies parallel to the sternum, on one or both sides, and extends from the sternoclavicular region and inserts variably on the xiphoid process or lower rib cartilage (1). The shape and size of the sternalis muscle is highly variable, and can be cord-like, flat, or irregular. Its exact function remains speculative, though it may play a role in the movement of the pectoral girdle where ipsilateral pectoralis major is hypoplastic (2). Clinically, the sternalis muscle is asymptomatic and is usually an incidental finding on imaging or post-mortem studies.
Epidemiology
The prevalence of the sternalis muscle varies widely in the literature, with reports ranging from 1% to 15% in cadaver studies (1). It is more commonly found unilaterally than bilaterally and more often found on the right versus the left. The prevalence between genders is roughly symmetric, though there may be a slight female predilection. There may be an increased incidence in patients of Asian descent.
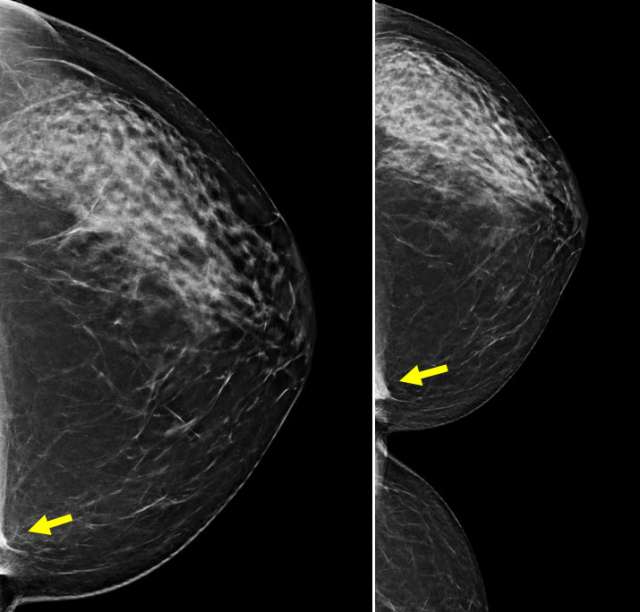
Mammographic Appearance
On mammography, the sternalis muscle presents as a variably shaped fibroglandular asymmetry on craniocaudal (CC) views, located in medial hemisphere at posterior depth (3). Sternalis muscles are not usually seen on mediolateral (ML) or mediolateral oblique (MLO) views. If the accessory muscle is incompletely visualized on the initial CC view, a cleavage view may be helpful to achieve better visualization. The appearance can mimic that of a skin lesion, lymph node, or other breast mass, potentially leading to misinterpretation.
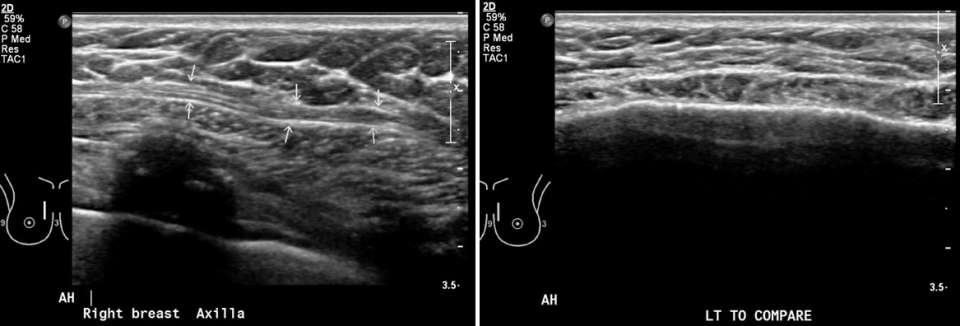
Ultrasound Appearance
Ultrasound imaging of the sternalis muscle reveals a well-defined, hypoechoic structure with internal striations, consistent with the appearance of skeletal muscle. Ideally, its continuity with chest wall muscles can be traced to prove muscular origin. In cases of suspected unilateral sternalis muscle, comparison ultrasound can be obtained of the contralateral chest to demonstrate asymmetry of the chest wall musculature.
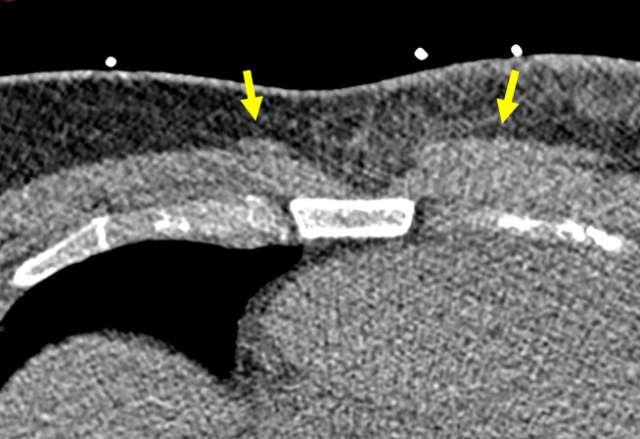
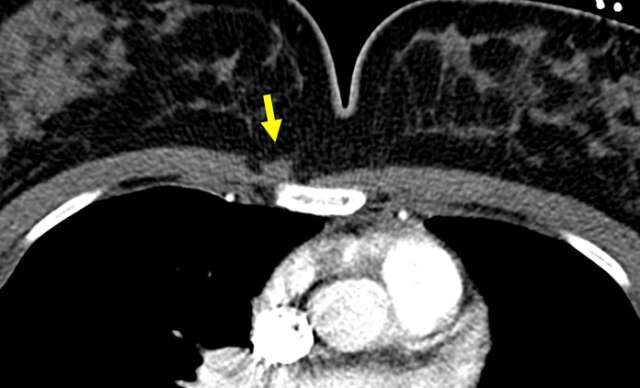
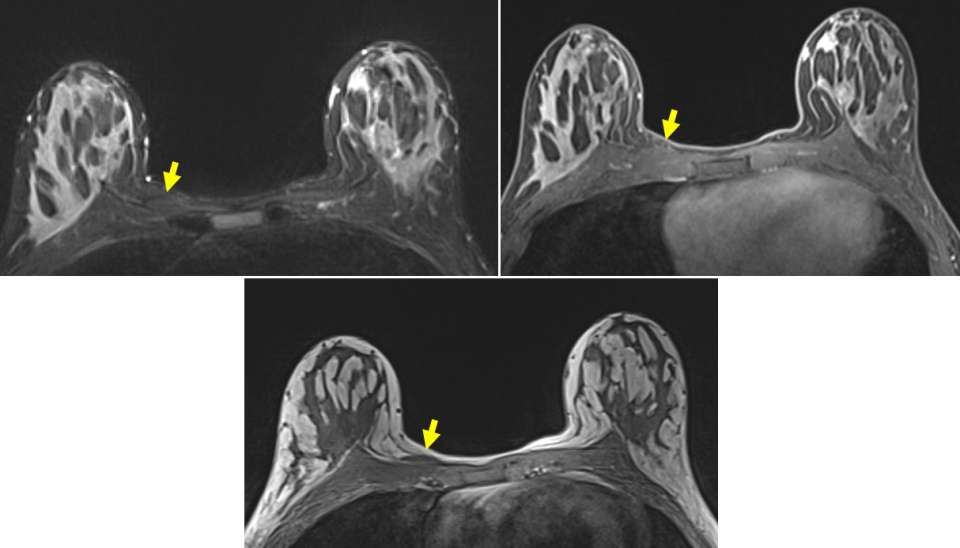
Magnetic Resonance Imaging and Computed Tomography Appearance
On MRI, the sternalis muscle demonstrates signal isointense to skeletal muscle. Likewise, CT scans depict the sternalis muscle as a well-demarcated structure with attenuation values similar to those of muscle, located anterior to the sternum. The shape is most often flat but can also be oblique or irregular (4). The presence of enhancing components on either MRI or CT is not typical and should prompt further evaluation or tissue sampling.
Clinical Significance
Recognition of the sternalis muscle as an anatomic variant can prevent unnecessary radiologic examinations, saving cost and preventing unwarranted patient distress. In addition to its radiological implications, proper identification of the sternalis muscle can help surgeons with pre-procedural planning if a muscle flap or sub-pectoral breast implant is planned (1). Detailed discussion of the surgical implications of the sternalis muscle variant is beyond the scope of this article.
References:
- Snosek M, Tubbs RS, Loukas M. Sternalis Muscle, What Every Anatomist and Clinician Should Know. Clin Anat. 2014 Sep;27(6):866-84. DOI: 10.1002/ca.22361. Epub 2014 Jan 16. PMID: 24431029.
- Gruber L, Martinoli C, Tagliafico AS, Gruber J, Klauser AS. A Rare Case of a Symptomatic Sternalis Muscle: Ultrasonograpy And MRI Correlation. Ultrasound Int Open. 2016 Nov;2(4):E140-E141. DOI: 10.1055/s-0042-113607. Epub 2016 Aug 24. PMID: 27896335; PMCID: PMC5120977.
- Demirpolat G, Oktay A, Bilgen I, Isayev H. Mammographic Features of the Sternalis Muscle. Diagn Interv Radiol. 2010 Dec;16(4):276-8. DOI: 10.4261/1305-3825.DIR.2733-09.2. Epub 2010 Aug 10. PMID: 20700868.
- Young Lee B, Young Byun J, Hee Kim H, Sook Kim H, Mee Cho S, Hoon Lee K, Sup Song K, Soo Kim B, Mun Lee J. The Sternalis Muscles: Incidence and Imaging Findings on MDCT. J Thorac Imaging. 2006 Aug;21(3):179-83. DOI: 10.1097/01.rti.0000208287.04490.db. PMID: 16915061.