Case: Simple Cyst, Clustered Microcysts, Complicated Cyst
by Madhu Joshi, MD, Fadi Dahoud, and Reza Fardanesh, MD
Introduction
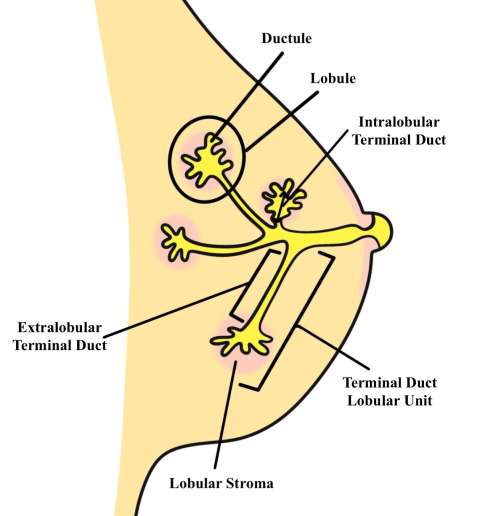
Breast cysts are common fluid-filled sacs that develop within breast tissue and typically arise along the terminal duct lobular unit. The exact cause of simple breast cysts is unknown; however, they likely develop in response to hormonal changes in the breast which can occur in the pre-, peri-, or post-menopausal period. Physiologically, distension of the tubule or obstruction along its course causes fluid to accumulate and eventually evolves into a sac-like structure that becomes a cyst.
Simple Cyst
Simple breast cysts are benign, fluid-filled lesions that do not have malignant potential. Simple cysts have characteristic features on mammography and ultrasound that allow definitive diagnosis.
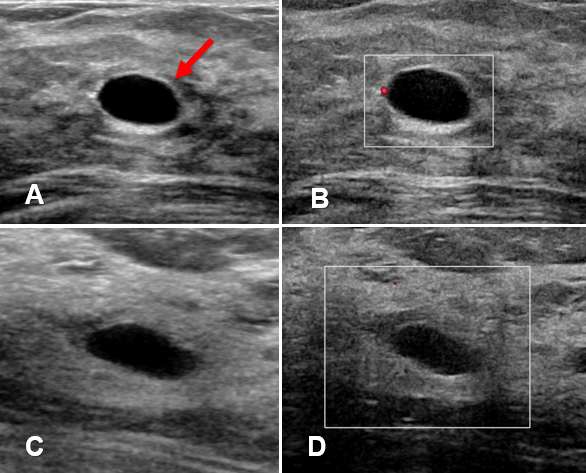
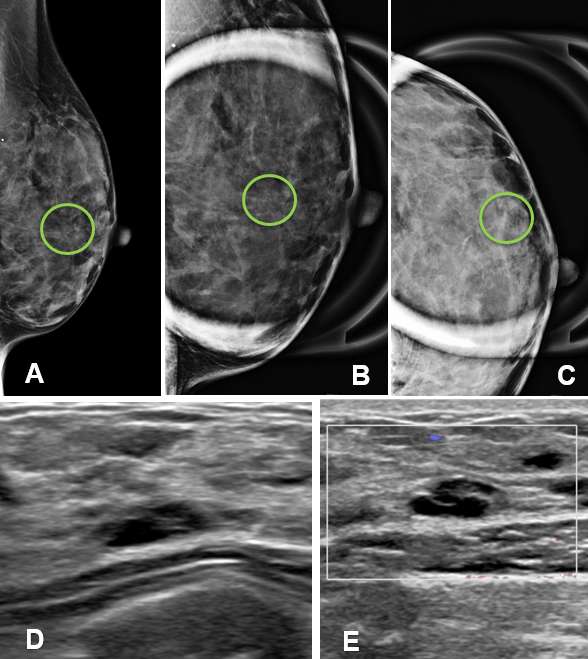
Ultrasound - Ultrasound is a particularly useful modality to evaluate breast cysts due to its ability to differentiate fluid-filled cysts from solid masses. Simple cysts appears as well-circumscribed, anechoic, round or oval structures, with thin walls that demonstrate posterior acoustic enhancement. Simple cysts can often be moved or compressed with the ultrasound probe which can help distinguish cysts from solid masses, which are usually immobile. Additionally, simple cysts do not exhibit vascularity nor contain internal echoes or solid components.
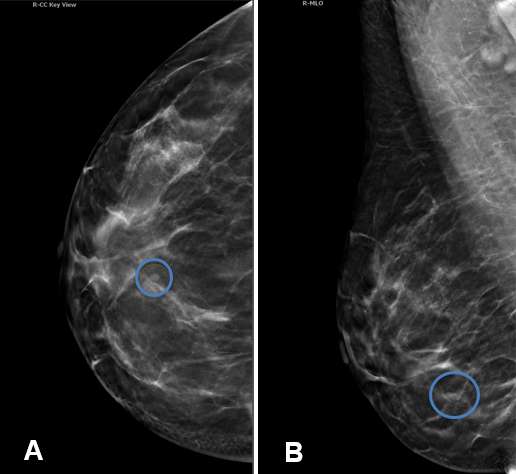
Mammography - Mammography often plays a complementary role in the assessment of simple breast cysts. They typically appear as well-circumscribed, oval or round, low density masses on mammogram. The density is often similar to that of surrounding fibroglandular tissue and background parenchymal elements are often discernible through the mass. Absence of associated microcalcifications and architectural distortion are additional reassuring features in differentiating a cyst from a solid mass.
Clustered Microcyst
Clustered microcysts are an additional form of benign, fibrocystic changes that can develop in the breast. They are often encountered in peri-menopausal women which is thought to be due to prolonged exposure to progesterone as the menstrual cycle shortens.
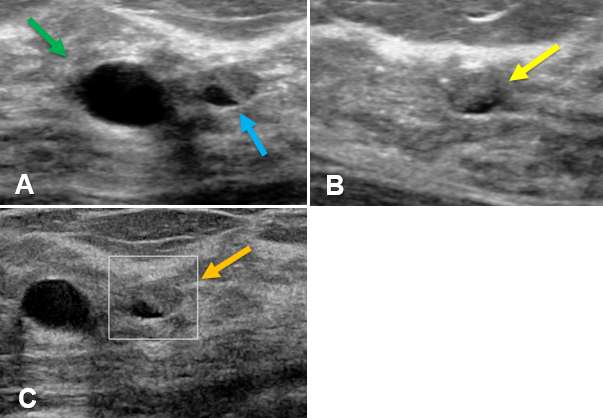
Ultrasound - On ultrasound, clustered microcysts display features similar to simple breast They typically appear as a group of small (2-3 mm) anechoic foci with thin (<0.5 mm) intervening septa and without a discrete solid component. Clustered microcysts also demonstrate posterior acoustic enhancement, similar to simple cysts. The margins of a clustered microcyst may be microlobulated but are well-defined.
Mammography - On mammography, clustered microcysts can appear as a focal round or oval mass with distinct margins that may be microlobulated. Similar to simple cysts, they can appear as relatively low-density lesions that allow background structures to be visualized through the mass. Calcifications may be present, which often reflect sediment/milk of calcium, however, they typically do not distort the surrounding parenchyma or cause architectural distortion. They may also appear an asymmetry or focal asymmetry or simply as a group of calcifications, which would warrant further evaluation with ultrasound.
Complicated Cyst
Complicated cysts are “probably benign” lesions as they contain internal debris which may mimic a solid mass appearance on imaging. The internal debris typically represents proteinaceous or hemorrhagic material which needs to be carefully evaluated in order to differentiate a complicated cyst from a complex cyst, which have malignant potential. Management of complicated cysts is dependent on the degree of suspicion and can either be closely followed with short-term interval imaging or undergo aspiration and/or biopsy for definitive diagnosis.
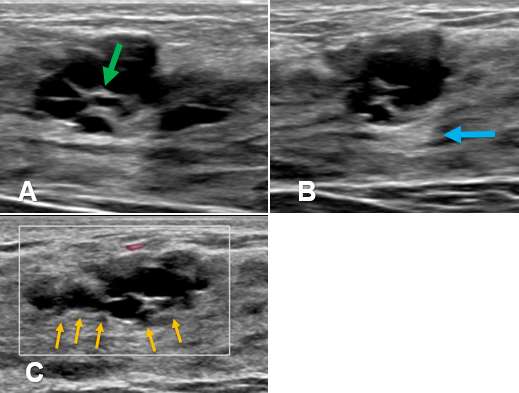
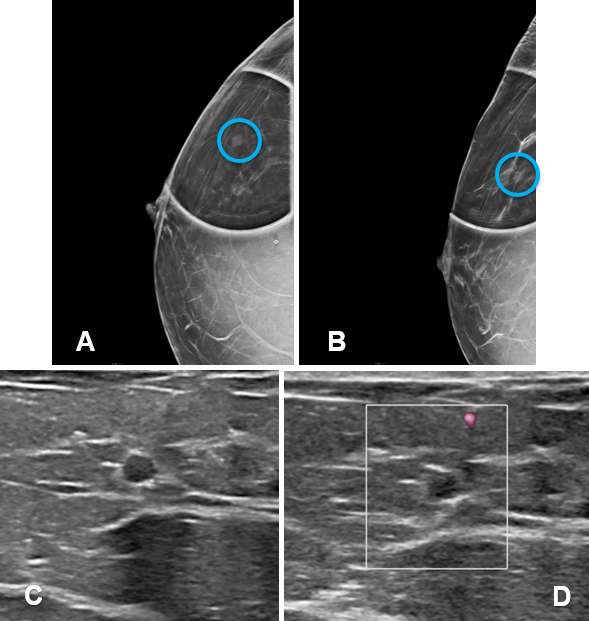
Ultrasound - On ultrasound, complicated cysts appear as round or oval lesions with thin walls, homogeneously hypoechoic internal debris, and may exhibit fluid-debris levels and low-level internal echoes that can change the shape of the cyst with changes in patient positioning. The internal debris may appear as hyperechoic components that adhere to the cyst wall and careful examination with power Doppler should be performed to exclude vascularity which would indicate a solid component. Complicated cysts may or may not exhibit posterior acoustic enhancement depending on the make-up of its internal components. The walls of a complicated cyst are often slightly thicker than that of simple cysts due to inflammation or mild fibrosis which can occur due to the internal proteinaceous or hemorrhagic components.
Mammography - Complicated cysts appear as well-circumscribed round, oval or slightly lobular, relatively low-density masses which may exhibit milk of calcium (layering) and rarely rim calcification.
References:
- Greenwood HI, Lee AY, Lobach IV, Carpentier BM, Freimanis RI, Strachowski LM. "Clustered Microcysts on Breast Ultrasound: What Is an Appropriate Management Recommendation?" AJR Am J Roentgenol. 2017 Dec;209(6):W395-W399. DOI: 10.2214/AJR.17.17813.
- Hines N, Slanetz PJ, Eisenberg RL. "Cystic Masses of the Breast." AJR Am J Roentgenol. 2010 Feb;194(2):W122-33. DOI: 10.2214/AJR.09.3688.
- Berg WA, Campassi CI, Ioffe OB. "Cystic Lesions of the Breast: Sonographic-pathologic Correlation." Radiology. 2003 Apr;227(1):183-91. DOI: 10.1148/radiol.2272020660.