Case: Fibroadenomas Tumors
by Sara Yang, MD and Nina Capiro, MD
Fibroadenomas are the most common benign solid mass occurring in the breast.1 They are tumors formed within the lobules of the breast tissue which consist of epithelium and stromal tissues.1 Although they may occur at any age, peak incidence is seen among adolescent and young women during the second and third decades of life.2 Fibroadenomas are stimulated by estrogen and progesterone, often growing during pregnancy and lactation with atrophy after menopause.3
Clinically, fibroadenomas may present as a palpable, mobile lump. When palpable, fibroadenomas are often described as smooth, firm, and rubbery.1 In about 15% of cases, patients may present with multiple fibroadenomas.1
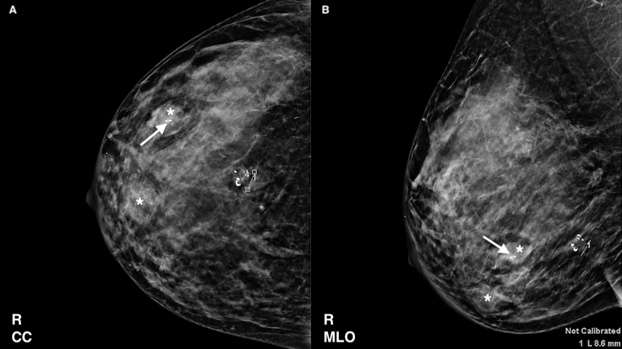
On mammography, fibroadenomas are typically well-circumscribed, round, oval or lobulated masses of varying sizes.1 They are often associated with so-called “popcorn calcifications”, which are coarse calcifications seen in involuting or hyalinizing fibroadenomas. When present, the diagnosis of a benign fibroadenoma can be made with certainty.1,4
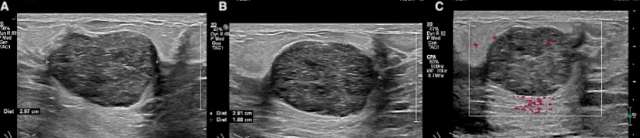
On ultrasound, fibroadenomas are usually well-circumscribed solid or oval masses that are homogenously isoechoic or hypoechoic.1 Fibroadenomas are often hypovascular and small, measuring less than 3 cm.5 Transmission characteristics are nonspecific as fibroadenomas can demonstrate either posterior acoustic enhancement or shadowing.1 As previously described, calcifications may be present. Occasionally, fibroadenomas may have non-circumscribed margins or show interval growth. In such cases, tissue sampling may be warranted to ensure diagnosis.6
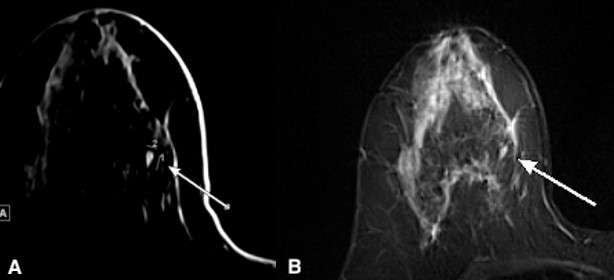
MRI is not necessary for the diagnosis of fibroadenomas. However, small fibroadenomas are often incidentally noted on MRI. Imaging features include T2 hyperintensity and homogenous enhancement with or without non-enhancing T1 hypointense fibrous septae.5
Fibroadenomas, if stable in size and asymptomatic, are generally managed conservatively with yearly clinical exams. Surgical management may be considered for symptomatic cases with pain or cosmetic deformity and for cases in which the size is greater than 5 cm.6
References
- Goel NB, Knight TE, Pandey S, Riddick-Young M, de Paredes ES, Trivedi A. "Fibrous Lesions of the Breast: Imaging-Pathologic Correlation." Radiographics. 2005 Nov-Dec;25(6):1547-59. DOI: 10.1148/rg.256045183. PMID: 16284134.
- Kuijper A, Mommers EC, van der Wall E, van Diest PJ. "Histopathology of Fibroadenoma of the Breast." Am J Clin Pathol. 2001 May;115(5):736-42. DOI: 10.1309/F523-FMJV-W886-3J38. PMID: 11345838.
- Sklair-Levy M, Sella T, Alweiss T, Craciun I, Libson E, Mally B. "Incidence and Management of Complex Fibroadenomas." AJR Am J Roentgenol. 2008 Jan;190(1):214-8. DOI: 10.2214/AJR.07.2330. PMID: 18094314.
- Mandell, Jacob. Core Radiology: A Visual Approach to Diagnostic Imaging. Cambridge University Press, 2013.
- Duman L, Gezer NS, Balcı P, Altay C, Başara I, Durak MG, Sevinç AI. "Differentiation between Phyllodes Tumors and Fibroadenomas Based on Mammographic Sonographic and MRI Features." Breast Care (Basel). 2016 Apr;11(2):123-7. DOI: 10.1159/000444377. Epub 2016 Mar 23. PMID: 27239174; PMCID: PMC4881274.
- Clark, HR, Merchant, KA, Omar, LA, Compton, LM, Hayes, JC. "Breast Lesions in Women Aged Younger than 30 Years: Clinical Presentation, Diagnosis, and Management." Journal of Breast Imaging, 2020 January/February; 2(1), 72-80. DOI: 10.1093/jbi/wbz086.